

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Although menopause is a normal process of aging in women, it is nevertheless a significant event in a women's life, accompanied by decrease in sex hormones and resultant physical and psychological changes.1
At the Stage of Reproductive Aging Workshop (STRAW) in 2001, menopause was defined within a seven stage of classification of a woman's reproductive aging. Reproductive stage was defined as the time from menarche to menopausal transition. Impending menopause amidst regular menstruation was termed as premenopause, which progressed to a stage of irregular menstruation, called as perimenopause. When menses has ceased for more than twelve months, a woman has entered the stage of postmenopause.1,2
Menopausal symptoms have individual variability in their presentations. These symptoms can be classified by the time of presentation into acute, subacute, and chronic. Acute symptoms include vasomotor symptoms (VMS) such as facial flashing and night sweats, insomnia, and depression. Subacute symptoms are mainly associated with uterovaginal atrophy. Chronic symptoms or sequelae of menopause include osteoporosis, cardiovascular disease, cerebrovascular disorder, and sexual dysfunction.3,4
VMS are the most common of the menopausal symptoms, experienced by 35-50% of women during perimenopause and 30-80% of women during the menopause stage. Overall, 75% of women over 50 years of age experience VMS. The duration of VMS is usually 1-2 years, although some women can experience it for even more than ten years.
In a survey conducted by the Korean Menopausal Society in 2001, of the 797 menopausal women (sample group), 89% had experienced menopausal symptoms, of which facial flushing was most common in 61% of women.5,6 A Gallup study of menopausal women in the United States (US) reported the four most common reasons for seeking medical care as facial flushing, night sweats, mood disorders, and insomnia.7
The etiology of VMS is thought to be the decrease in systemic estrogen and symptoms are most prominent during early menopause when estrogen levels fall acutely. The symptoms usually last for 1-2 years, but in 25% of women, VMS continue for 5 years, and can extend beyond 10 years in about 10% of menopausal women.5
With increasing life expectancy, postmenopausal stage will also increase in length in a woman's lifecycle. According to the Organisation for Economic Co-operation and Development (OECD) health data (2008), Korean women's life expectancy is 82.4 years. This is 13th of the 30 member countries, surpassing the group average of 81.7 years. The average age at menopause for Korean women has been reported to be 49.7 years.6 Assuming that these numbers are not grossly erroneous, an average Korean woman will spend about 30 years and more than a third of her life in the post-menopausal stage. Needless to say, we can expect that an increasingly greater proportion of our clinical visitors will be the elderly. Beforehand, we need to be more familiar with the physiological and psychological changes as well as the medical need, which the menopausal women require.
Ethnic differences exist in the experience of menopause. According to Spector's definition of ethnicity,8 which is a cultural group's sense of identification associated with the group's common social and cultural heritage, Korea is homogenous in ethnic composition.
This study aims to complement the information gathered from previous studies conducted on Korean menopausal women, with an emphasis on subjective experiences, to help the clinicians to better understand the women's journeys through menopause.
Materials and Methods
1. Study participants
Healthy perimenopausal and menopausal Korean women between the ages of 40 to 60 years were included in the study. Survey participants were recruited from four Korean provinces, Seoul, Busan, Daegu, Gwangju, and Daejeon. The percentage of each province was decided according to the Korean population study conducted in 2010. We used multi-level stratification based on age and geographic location, and then conducted random sampling.
The study included both clinician diagnosed as well as self-diagnosed women with perimenopause or menopause. Diagnosis of perimenopause was based on cessation of menses for less than 12 months, showing variation in menstrual cycle that exceeds 7 days from one's normal menstrual cycle, irregular cycle with absence of 2 or more menstruation, or irregular cycle, which became regular with medication. Menopause was diagnosed as cessation of menses for over 12 months, regular cycle with medication but with no menses for over 12 months before treatment.
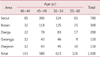
The study aimed to capture a sufficient sample to be representative of the menopausal and perimenopausal population in Korea. According to "The Pan-Asia Meonpause study (PAM study)" published in 2005, in Korean menopausal women between 40 and 65 years of age, facial flashing prevalence was reported to be 47.4%, and night sweats were experienced in 34.0% of women.9 We selected a number in the middle of these two figures as the predicted prevalence of VMS (40.7%) and approximated a sample size of 1500. The sample size calculation was based on the following equation: sample size (n) = Z2 × p (1-p) / D2 (Z = 1.96; p = prevalence of disease; D = 2.5%). Z is the standard score corresponding to 95% confidence interval and p is prevalence of 40.7%. The margin of error (D) was set at 2.5%. Table 1 shows the geographic distribution of the 1,500 women.
2. The survey
Those who agreed to be surveyed were questioned face to face by trained interviewers. The survey collected 1) general information including date of birth, height, weight, education, marital status, job, and monthly income, 2) subject and family medical history, 3) lifestyle habits including smoking, alcohol, caffeine, physical exercise, and amount of perceived stress, 4) reproductive history including menarche, pregnancy, delivery, abortion, contraception, current menstrual state, perception of menopause, and menopausal symptoms, 5) treatment history for menopausal symptoms, including type of management, and reason for choice, 6) quality of life, and 7) VMS including characteristics of symptoms, and treatment history.
The Korean version of the Menopause Rating Scale (MRS) was used to investigate the prevalence of menopausal related symptoms and the Korean version of Women's Health Questionnaire (WHQ) was used to assess quality of life. MRS is a well known tool for the assessment of health related quality of life of women in climacteric state and is now available in 9 language versions including Korean.10,11 The WHQ was designed to measure possible changes in health and well-being during menopausal transition and asks the woman to rate her perception of emotional and physical health.12
For questionnaires associated with treatment behavior and the reason for seeking treatment, multiple answers were allowed.
Results
Among the 1,500 women, 66% were classified as perimenopause, 28% as menopause (20% early menopause: < 5 years from cessation of menses, 8% late menopause: > 5 years), and 7% had undergone hysterectomy. With respect to age group, among women between ages 40-44 years, and 93% were perimenopausal. The percentage of premenopausal women between the ages of 45-49, 50-54, and 55-60 were 87%, 51%, and 6%, respectively.
About 41.6% of women in perimenopause reported having experienced VMS in recent six months, 53.1% of women in early menopause and 36.5% of women in late menopause (50% overall in the menopause group) had experienced VMS in the past six months. Thirty point six percent of women with hot flashes, and 27.9% of women with sweating responded that these symptoms were not related to menopause.
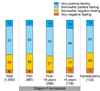
Overall subjective perception of menopause was positively associated with duration of menopause (Fig. 1).
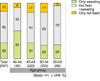
Distribution of VMS is displayed by age group (Fig. 2).
In the 556 women who experienced hot flashes, the mean symptom duration was 18 months. Distribution of symptom duration, frequency and single episode length are displayed in figure 3.
In the 470 women who experienced sweating, the mean symptom duration was 17 months. Frequency of sweating, and night sweats are shown in figure 4.
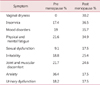
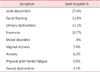
In the late menopause group, the reported experiences of symptoms pre- and post-menopause are shown in Table 2. Comparing pre and post menopause symptoms in late menopause women, vaginal dryness increased the most by 30%. Sleeping disturbance, mood disorders, physical and mental fatigue, sexual problems, irritability, joint and muscle pain were all increased after menopause. However, anxiety symptoms and urinary problems seemed to decrease after menopause.
The symptoms that promoted menopausal women to seek medical care are shown in Table 3.
Seventy percent of women experiencing VMS were actively addressing the symptoms. Most common reasons for seeking treatment were symptom relief (64%), to maintain current health (60%), and the least common reason was because others were seeking treatment (7%). Forty-two point six percent reported use of nutritional supplements, 31.8% exercised, 25.1% tried special diet, 13% sought medical care, 10% had tried hormone therapy, 6% were treated by oriental medicine, and 30.7% reported doing nothing to address VMS.
Over 90% reported being satisfied with their treatment option. Ninety-three percent of those who used oriental medicine were satisfied with the treatment results, 80% were satisfied with nutrition supplements, and 74% with change in diet.
In women who did not seek any treatment, 45% answered that menopause is a natural part of life and not something to be treated, while 42% stated that symptoms were not severe enough to warrant active treatment. Nine percent had other reasons including being too busy to seek help, no idea as how to seek treatment, do not consider it as menopausal symptoms, thought treatment is not likely to be effective, and do not want to be dependent on medication.
Discussion
Menopause in its entirety is a subjective experience. It is a complex integration of physiological changes associated with aging and changes in sex hormones interacting with the meaning of menstruation and what menopause symbolizes for each individual woman in their variable sociocultural environments. We were interested in learning about how women experience menopause.
As much as menarche seems to have different meaning in context of Korean cultural when compared to Western culture, it is generally believed that menopause would be experienced differently. Korean girls experience menarche in silence, in a clandestine manner, often undisclosed to the men in the family including her father. Girls are often told that beginning of menarche means beginning of hardship, probably stemming from historical meaning of marriage for a woman, who held most if not all household responsibilities including ancestral rites commemorating death anniversaries of ancestors, which involved many days of laborious preparation. From what we understand from Western culture, menarche is openly celebrated as a girl enters the life of a woman. Western psychoanalytic thoughts have emphasized the importance of sexual activities in life fulfillment and perhaps menarche symbolizes rites of passage into this search of fulfillment.
Just as menarche is experienced privately, menopause seems to be experienced privately by Korean women. Menopausal women in Korea rarely present with complaints of VMS or vaginal dryness. Rather, they most often present with somatic complaints such as fatigue, pain, low energy, sleep problems, concerns about potential bone and cognitive health problems. Our data show that a large portion of Korean women did not recognize facial flashing and sweating as menopausal symptoms. In a culture, that readily acknowledges somatic ailments as deserving attention, but seeking help for natural processes such as menopause or subjective experiences such as depression as characterological flaws, it is not surprising that there is low awareness about menopausal symptoms. How best to educate the public and medicalize treatable discomforts of menopause is a challenge, which clinicians should try to tackle.
The overall perception of menopause was increasingly positive with age. This could be because Korean women live in a culture that respect the elderly, and welcome this phase of life where she is freed from the burden of menstruation, while acquiring enhanced status in the family and society. It is generally believed that Asian women experience fewer menopausal symptoms and cultural views allow Asian women to embrace menopause with a tranquil acceptance as another milestone in life.13,14 The prevalence of hot flashes in Asian menopausal women is 10-20% when compared to 30-50% in Western women.14,15 The Study of Women's Health Across the Nation (SWAN) study noted that Asian women report less significant symptoms than Caucasians and African Americans.
The SWAN also noted that some groups of women were more likely to experience VMS and more severe symptoms. The study reported increased symptom reporting among women with less education, homemakers, those who had difficulty paying for the basic necessities of life, and those of larger body size.16 There was no such trend observed in our study. However, looking at the demographic distribution, most of the participants in our study (92%) had at least high school graduation level education and the majority (86%) of the sample had normal body mass index (BMI) of less than 25. Our demographic distribution did not allow adequate sample size to reflect variation according to socio-economic status.
A potential difference in Korean menopause is the earlier onset when compared to those in Western countries or even neighboring East Asian countries. According to Kim and Choi3 the average age of menopause in Eastern Asia was 51.09 years, US 51.3 years, Netherlands 51.2 years, and Korea 49.3 years. Our data in Korean women show similar results, with 49 years as an average age of onset of menopause. There is no scientifically plausible explanation for this observation as other physical signs of aging such as decrease in skin turgor, and increase in flabby adiposity, are generally delayed in Koreans. Perhaps an anthropological reason should be fetched to explain this observation.
In examining the symptom distribution by age group, younger women experienced predominantly only hot flashes while the majority of older women experienced both hot flashes and sweating, thus raising the questions whether menopausal symptoms evolve from hot flashes to sweating.
There are some limitations in interpreting the data presented in Table 2, the symptoms, which women experienced as menopause, due to potential recall bias. People are more likely to remember more recent experiences of discomfort than those experienced several years ago. It could be possible that functional disturbances associated with symptoms may affect recall. For example, vaginal dryness was only reported to have occurred after menopause and not during premenopausal phase. This symptom, which accounted for 7.4% of the reason for seeking treatment, is likely to have been only intermittently distressing. In contrast, joint discomfort, which is likely to have been more chronically disabling, appears to have better recalled as well as treatment sought more often.
The most common reason for seeking treatment in our sample was joint discomfort. Non-VMS such as body and joint aches and sleeplessness have been reported to be more prevalent in Asian women.14 Although vaginal dryness was one of the more common symptoms experienced in the menopause, very few sought treatment. Vaginal dryness or loss of sexual desire was regarded as less important by Asian women as they did not associate sexual function with self-confidence.14
Of note is the discordance between the frequency of mood and anxiety symptoms experienced during premenopausal and menopausal phases and the proportion of women seeking treatment for psychological distress. This could be because the severity of these symptoms is not disabling. Alternatively, Koreans may be experiencing depression and anxiety in a culture-bound fashion in which somatic symptoms predominate.17
Since the WHI scare, the choice regarding which menopausal symptoms to manage with which treatment option is primarily consumer-driven. Understanding the complexities involved in a woman's individual experience of menopause would be important for the clinicians during counseling women seeking treatment.


 XML Download
XML Download