

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
The most common anatomic location of calcific tendinitis is the suprasupinatus muscle of the shoulder joint. However, it is known to develop in any joint including the hip, knee. Infarction of skeletal muscle in the distal areas of the limbs due to vascular occlusion is a well recognized systemic condition in patients who have diabetes. The author experienced mass-like lesion combined muscle infarction and calcification within pure semitendinosus tendon without diabetes in posterosuperior area of distal thigh in old age.
Figures and Tables
 | Figure 1Lateral radiograph of right knee show calcified lesion (arrow) on posterior area of distal femur.
|
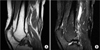 | Figure 2Magnetic resonance images shows well-defined soft tissue mass along semitendinosus tendon, posterior aspect of distal thigh. (A) T1-weighed image: slightly high signal intensity (B) T2-weighed image: heterogeneous iso signal intensity.
|
 | Figure 3Gross examination reveals tendon (right white portion) with skeletal muscles (left cut view).
|
 | Figure 4Microscopic findings of tendinitis with muscle infarct. (A) Low power view reveals tendon (T) and skeletal muscle (M) (×40). (B) Degeneration with infract (arrows) was noted in muscle portion (×200, H&E). (C) Degeneration with calcification (arrows) was noted in tendon portion (×100, H&E). (D) Tendinitis with foreign body reaction (arrows).
|
References
1. Uhthoff HK, Sarkar K, Maynard JA. Calcifying tendinitis: a new concept of its pathogenesis. Clin Orthop Relat Res. 1976. (118):164–168.
2. Gärtner J, Simons B. Analysis of calcific deposits in calcifying tendinitis. Clin Orthop Relat Res. 1990. (254):111–120.
3. Baudrillard JC, Lerais JM, Segal P, et al. Enthesopathy of the upper insertion of the musculus rectus femoris. A retrospective sign of tendon rupture in sports pathology. J Radiol. 1986. 67:185–191.
4. Tennent TD, Goradia VK. Arthroscopic management of calcific tendinitis of the popliteus tendon. Arthroscopy. 2003. 19:E35.
5. Aboulafia AJ, Monson DK, Kennon RE. Clinical and radiological aspects of idiopathic diabetic muscle infarction Rational approach to diagnosis and treatment. J Bone Joint Surg Br. 1999. 81:323–326.
6. Damron TA, Levinsohn EM, McQuail TM, Cohen H, Stadnick M, Rooney M. Idiopathic necrosis of skeletal muscle in patients who have diabetes. Report of four cases and review of the literature. J Bone Joint Surg Am. 1998. 80:262–267.
7. Lauro GR, Kissel JT, Simon SR. Idiopathic muscular infarction in a diabetic patient. Report of a case. J Bone Joint Surg Am. 1991. 73:301–304.
8. Hinton A, Heinrich SD, Craver R. Idiopathic diabetic muscular infarction: the role of ultrasound, CT, MRI, and biopsy. Orthopedics. 1993. 16:623–625.
9. Morcuende JA, Dobbs MB, Crawford H, Buckwalter JA. Diabetic muscle infarction. Iowa Orthop J. 2000. 20:65–74.
 XML Download
XML Download