

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Purpose
The purpose of this study is to compare general survival rate and survival rate according to expectable prognostic factors by analyzing the result of treating a patient of squamous cell carcinoma.
Materials and Methods
From Mar. 1999 to Feb. 2011, 151 patients were pathologically confirmed as squamous cell carcinoma of limbs and body in our hospital, and among those patients, 51 patients underwent the surgical treatment. This study included 41 patients who underwent the surgical treatment and were followed-up for more than 12 months. The mean age of population was 64.4 years. 31 males and 10 females were included. Wide excision with following skin grafts or flaps for reconstruction (29 cases) was mostly performed, but amputation (12 cases) was also performed for cases with extremities where resection margin was difficult to obtain and cases with neural or vascular invasion. 8 patients underwent chemotherapy or radiotherapy after resection, and 33 underwent the operation only. Stages were classified by AJCC Classification, survival rate was calculated by Kaplan-Meier method and survival rate of groups was compared by Log-rank test. For the expectable prognostic factors related to survival rate, location of primary lesion, cause of disease, pathologic grade, staging, surgical method, additional anticancer therapy were examined and each survival rate was compared.
Results
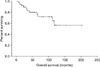
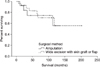
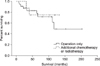
The average follow-up period was 65.2 (12-132) months. Thirty patients survived out of 41 patients till last follow up. The overall survival rate in 5 years was 77%. Three cases (7.3%) had local recurrence, and 7 cases (17.0%) had metastasis. The average period of recurrence from operation was 27 (18-43) months. Possible prognostic factors such as location of primary lesion, cause of disease, pathologic grade, staging, additional anticancer therapy showed no significant difference in survival rates. However, patients with amputation showed significantly lower survival rate than those with wide excision.
Figures and Tables
 | Figure 1(A) Forty one-year old male got an open wound on his left buttock 5 years ago, and that was not healed so far. It was diagnosed as squamous cell carcinoma at a local clinic. (B) Wide excision was done. (C) Local transposition flap on left thigh, meshed skin graft was done.
|
 | Figure 2(A) Fifty year-old male had suffered from post-burn scar contracture from right axilla to forearm, and marjolin's ulcer of right forearm since he got burned 40 years ago. They were diagnosed as squamous cell carcinoma at a dermatologist's office. (B) Above-elbow amputation, and release of burn-scar contracture on right axilla was done. (C) Skin graft was done.
|
 | Figure 4Kaplan-Meier graph for survival rate of the acral and proximal location of squamous cell carcinoma.
|
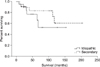 | Figure 5Kaplan-Meier graph for survival rate of the idiopathic and secondary cause of squamous cell carcinoma.
|
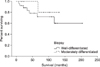 | Figure 6Kaplan-Meier graph for survival rate of the well-differentiated and moderately-differentiated grade of squamous cell carcinoma.
|
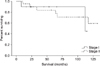 | Figure 7Kaplan-Meier graph for survival rate of the stage I and stage II of squamous cell carcinoma.
|

References
1. Johnson TM, Rowe DE, Nelson BR, Swanson NA. Squamous cell carcinoma of the skin (excluding lip and oral mucosa). J Am Acad Dermatol. 1992. 26:467–484.
2. Chung HG, Moon TK, Bang DS, Lee MG. Clinical observation of cutaneous malignant tumors and premalignant lesions over 15 years (1982-1996). Korean J Dermatol. 1999. 37:1413–1422.
3. Chuang TY, Popescu NA, Su WP, Chute CG. Squamous cell carcinoma. A population-based incidence study in Rochester, Minn. Arch Dermatol. 1990. 126:185–188.
4. Lardaro T, Shea SM, Sharfman W, Liégeois N, Sober AJ. Improvements in the staging of cutaneous squamous-cell carcinoma in the 7th edition of the AJCC Cancer Staging Manual. Ann Surg Oncol. 2010. 17:1979–1980.
5. Sedlin ED, Fleming JL. Epidermoid carcino-ma arising in chronic osteomyelitis foci. J Bone Joint Surg [Am]. 1963. 45:827–838.
6. Arons MS, Lybch JB, Lewis SR, et al. Scar tussue carcinoma, a clinical study with special reference to burn scar carcinoma. Ann Surg. 1965. 161:170–188.
7. Cheney ML, Varvares MA. Recognition and management of the high-risk cutaneous squamous cell carcinoma. Curr Probl Dermatol. 1993. 5:141–192.
8. Goldman GD. Squamous cell cancer: a practical approach. Semin Cutan Med Surg. 1998. 17:80–95.
9. Kwa RE, Campana K, Moy RL. Biology of cutaneous squamous cell carcinoma. J Am Acad Dermatol. 1992. 26:1–26.
10. Jeon DG, Lee JS, Kim SJ, et al. Role of surgery in squamous cell carcinoma. J Korean Bone Joint Tumor Soc. 1998. 4:30–36.
11. Rowe DE, Carroll RJ, Day CL Jr. Prognostic factors for local recurrence, metastasis, and survival rates in squamous cell carcinoma of the skin, ear, and lip. Implications for treatment modality selection. J Am Acad Dermatol. 1992. 26:976–990.
12. Hahn SB, Kim DJ, Jeon CH. Clinical study of Marjolin's ulcer. Yonsei Med J. 1990. 31:234–241.
13. Gallagher RP, Ma B, McLean DI, et al. Trends in basal cell carcinoma, squamous cell carcinoma, and melanoma of the skin from 1973 through 1987. J Am Acad Dermatol. 1990. 23:413–421.
14. Brodland DG, Zitelli JA. Surgical margins for excision of primary cutaneous squamous cell carcinoma. J Am Acad Dermatol. 1992. 27:241–248.
15. Norman J, Cruse CW, Espinosa C, et al. Redefinition of cutaneous lymphatic drainage with the use of lymphoscintigraphy for malignant melanoma. Am J Surg. 1991. 162:432–437.
16. Mohs FE. Chemosurgery: Microscopically controlled surgery for skin cancer. 1978. Springfield, IL: Charles C Thomas.
 XML Download
XML Download