

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Skip lesion is not uncommon feature in osteosarcoma and considered to be importantly associated with poor prognosis factor, and thus, should be excised with the main mass. The accurate pre-operative evaluation of the intramedullary extent of osteosarcoma is essential, because it determines the level of bone resection. Among the reliable detection methods, bone scan has a drawback of high rate of false negative results and regional MRI has a difficulty to cover the whole involved lesions without clinical suspicion. The authors report a case of osteosarcoma of the distal femur with a proximal skip lesion that was not detected by either regional MR imaging or by bone scan, but which was visualized by FDG-PET/CT.
Figures and Tables

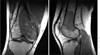 | Figure 2Coronal and sagittal T1-weighted MR image at presentation show an osteosarcoma extending approximately 10 cm from the distal femoral articular surface. There is some soft tissue extension in medial direction.
|
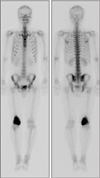 | Figure 3Whole body bone scan at presentation showing isolated area of increased uptake in medial aspect of right distal femur. There is no suspected metastatic and skip lesion.
|


References
1. Enneking WF, Kagan A. "Skip" metastases in osteosarcoma. Cancer. 1975. 36:2192–2205.
2. Enneking WF, Kagan A. The implications of "skip" metastases in osteosarcoma. Clin Orthop Relat Res. 1975. (111):33–41.
3. Wuisman P, Enneking WF. Prognosis for patients who have osteosarcoma with skip metastasis. J Bone Joint Surg Am. 1990. 72:60–68.
4. Cheon GJ, Chung JK, Kim YK, et al. Comparasion of whole body F-18 FDG PET and Tc-99m MDP bone scan for the assessment of metastatic bone lesions. World J Nucl Med. 2003. 2:18–29.
5. Gosheger G, Gebert C, Ahrens H, Streitbuerger A, Winkelmann W, Hardes J. Endoprosthetic reconstruction in 250 patients with sarcoma. Clin Orthop Relat Res. 2006. 450:164–171.
6. Grimer RJ. Surgical options for children with osteosarcoma. Lancet Oncol. 2005. 6:85–92.
7. Ardran GM. Bone destruction not demonstrable by radiography. Br J Radiol. 1951. 24:107–109.
8. Berquist TH. Magnetic resonance imaging of primary skeletal neoplasms. Radiol Clin North Am. 1993. 31:411–424.
9. Basu S, Alavi A. Bone marrow and not bone is the primary site for skeletal metastasis: critical role of [18F]fluorodeoxyglucose positron emission tomography in this setting. J Clin Oncol. 2007. 25:1297. author reply 1297-9.
10. Hur J, Yoon CS, Ryu YH, Yun MJ, Suh JS. Accuracy of fluorodeoxyglucose-positron emission tomography for diagnosis of single bone metastasis: comparison with bone scintigraphy. J Comput Assist Tomogr. 2007. 31:812–819.
 XML Download
XML Download