

 PDF
PDF ePub
ePub Citation
Citation Print
Print


A turret exostosis was first described by Wissinger et al.1) in 1966. A rare complication after trivial injuries to the dorsum of the proximal and middle phalanges of the fingers. As the lesion enlarges, the patient complains pain and a palpable mass, which may cause disruption in the extensor mechanism, resulting in the loss of finger flexion.2)
Almost all turret exostosis that reported involve middle and distal phalanx, but we experienced a peculiar turret exostosis involve metacarpus.
Case Report
A seventy-five-year-old man presented with a palpable mass without pain of the right hand, which had been gradually enlarging over a ten-year period. On physical examination, a 3×3-cm non-tender mass was observed on the dorsoulnar aspect of the fifth metacarpal area. The mass was round shaped with irregular surface, firm and fixed with negative Tinel's sign. Flexion of the ring finger was limited. The initial hand radiographs demonstrated a large soft tissue mass with ossification from the fifth metacarpophalangeal (MCP) joint to mid-shaft of the fifth metacarpal bone (Fig. 1). A whole body bone scan revealed that the patient had an active heterotopic ossification lesion (Fig. 2A). We applied outpatient follow-up and symptomatic treatment and observed progress. In plain radiography after 6 months, the size of the mass had not been changed, and whole body bone scan showed a decrease in contrast enhancement by over 50% compared to theat in the previous scan (Fig. 2B).
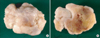
The operation started with a skin incision of dorsal aspect and the mass was observed on the MCP joint, neck and shaft of the metacarpal bone. Intraoperative finding demonstrated a sessile type, white colored and round shaped hard mass sized at 3.5×2.5×2-cm. The mass consisted of bone, cartilage cap and capsulated fibrous fascia (Fig. 3). Histopathological finding was consistent with exostosis (Fig. 4). After one week of surgery, the patient had full range of motion of the little finger. At the time of final follow-up one years and six months after the excision, the patient maintained full range of motion of the little finger and the hand radiographs showed no evidence of recurrence of the turret exostosis (Fig. 5, 6).
DISCUSSION
A turret exostosis is a rare complication after trivial injuries to the dorsum of the proximal and middle phalanges of the fingers.1) The differential diagnosis includes benign lesions, such as osteochondroma, and malignant neoplasms, such as osteosarcoma and osteochondrosarcoma.2) Most frequently involved sites are the index and the little finger,3) but rarely involve the thumb,2) metacarpal,3) big toe3) and talus.4) To our knowledge, a turret exostosis involving the metacarpal has been reported one case in the hand and orthopaedic literature by Rubin et al.2) According to that report, the exostosis involving fifth metacarpal had recurred on one-year follow-up clinical and X-ray examination. In our case, turret exostosis of the fifth metacarpal, no evidence of recurrence was not found on clinical and X-ray follow-up after a year and six months after the surgery.
The treatment of choice for a turret exostosis is excision appropriately timed to the maturation of the lesion.3) Wissinger et al.1) recommended that excision should not be performed less than four to six months after the original injury. Premature excision and poor surgical technique may invite recurrence.1) At surgery, if sufficient time has elapsed from the original injury, the planes will be clearly defined between the lesion, the overlying periosteum and the underlying cortex.2)
We used bone scan study as a modality to set the time of operation for turret exostosis. Our case showed a marked decrease in the bone uptake of the lesion in bone scan performed after 6 months follow-up from the initial bone scan study. So surgical removal was performed and obtained satisfactory results without recurrence.
It seems that there is no established examination protocol so far. In order to set the time of operation, it seems helpful to perform Metacarpusbone scan after an injury on a finger or hand during the early period when a radiologically ectopic bone lesion develops. In general, if bone scan after 6 months from the injury shows the increase of lesion intake by over 50%, we may consider operation.





 XML Download
XML Download