

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
As the largest health profession, the nurse workforce plays an important role in the delivery of quality health-care services and productivity in health-care organizations. Nursing is the profession that interacts the most closely with clients in the health-care sector, and therefore, requires the cooperation of health-care staff, reciprocal communication, and team work [1]. Currently, some cooperative behaviors have emerged among co-workers in hospital organizations and these behaviors have gradually gained much more importance. The organization members perform these behaviors during their fulfillment of organizational roles in order to improve healthy work environments [2]. Organization citizenship behavior (OCB) is one type of extra role behaviors, which increases tendencies towards helping and sharing information, promoting a feeling of conscience, tolerance, and praising the institution [3]. OCB comprises positive social behaviors that increase the efficiency of an organization as a whole. Moreover, OCB is characterized as the behavior of individuals in an organization and defined as extra role behaviors, rather than defined roles and responsibilities [4]. These are behaviors displayed voluntarily by workers, dependent on their personal choice, without a written obligation, and they are not clearly indicated in the agreement of an organization and are not required by a job description [4]; therefore, negligence in these behaviors does not bring any penalty.
For these reasons, OCB is essential for establishing more reciprocal communication and cooperation among health-care staff, managers, and other workers to promote better patient outcomes and successful health-care organizations [3]. Nurses, who are the most active members of the health-care staff, should display high levels of OCB in order to more efficiently provide nursing care [5]. However, nurses who do not display OCB are more inclined to demonstrate negative behaviors related to reduction in nursing care service quality and a lack of sharing among team members. Nurse managers should try to enhance nurses' OCB to meet the demands and expectations of clients and facilitate a high work-team spirit. They should be able to work together with others in coordination and perform the requirements of OCB in their institutions [3]. Nurse managers should determine the OCB levels of nurses and effective factors.
Leadership of nurse managers is an important factor contributing to successful behavioral transformation [6]. Transformational leadership shapes nurses' behavior and prepares them to be competitive. Transformational leadership behavior (TLB) has received increased attention in terms of its relationship with the OCB of nurses. Bass and Avolio [7] argued that transformational leadership motivates followers to exceed expectations by causing them to realize the importance of specific goals and subsume their own interests to organizational interests, as well as further motivating them to feel a need for achievement, growth, and self-actualization. Transformational leadership encourages OCBs that are voluntary and not directly connected to an organizational reward system, but which contribute to improving organizational effectiveness and climate [1]. Researchers found a positive impact of transformational leadership on OCB, especially with regard to helping behaviors [4], organizational compliance [8], and civic virtue [9]. When nurse managers serve as role models of transformational leaders and give special attention to each nurse's needs and shared goals, their behaviors encourage nurses to follow and engage in self-sacrificing behaviors characteristic of OCB [910]. One study found only a direct effect between TLB and OCB [4], while other studies reported indirect effects between the same variables [1112]. Given the inconsistent results, more research is needed to investigate the relationship between TLB and OCB.
Nurses who share networks of social relationships at work perceive them to be meaningful and challenging. Thus, the chances of a socially empowered nurse performing well and conforming to OCB are higher. Research suggests that social capital improves the members' capacity to share knowledge and skills through their networks to accomplish organizational goals [13]. With respect to the nursing care sector, social capital has a positive effect on organizational outcomes [5]. Social capital has been defined as the sum of the actual and potential resources derived from the network of relationships possessed by a social unit [14]. Networks of social relationships at work include relationships with other nurses, health-care professionals, or patients, to obtain power and authority for oneself. Social capital refers to the social complexities that are reciprocally connected within specific social structures marked by trust, networks, and norms [15]. It promotes work motivation by increasing the sense of unity in an organization and improves the organization's efficiency by promoting cooperation between individuals and groups [2]. If effectively established, an infrastructure that helps members actively interact can be developed, creating a driving force for building intellectual capital. Social capital is an important mediator that affects OCB [5]. It is not an innate trait, but can be changed through organizational training programs [5]. Although the feasibility of social capital is being assessed in the field of nursing workforce management, no research has focused on the relationships among TLB, social capital, and OCB.
Therefore, the findings in this study yield basic data related to building a workforce management plan to increase OCB turnover by identifying whether social capital plays a mediating role in the relationship between TLB and OCB.
METHODS
1. Study Design
This cross-sectional descriptive survey aimed at identifying the mediating effect of social capital in the relationships between TLB and OCB in nurses.
2. Participants and Data Collection
The participants in this research were registered nurses working at two university-affiliated teaching hospitals in a metropolitan city of South Korea. The study data were collected between March 21 and April 15, 2016. Initially, 250 participants were recruited using convenience sampling. The calculation of sample size was based on the formula proposed by Faul and colleagues [16] using G*Power 3.1.2 software. A total of 180 participants were required to detect an effect (α=.15) with a power (1-β) of .95 and a two-tailed α of .05 for the regression analysis with a maximum number of independent variables. Assuming a 20.0% wastage rate, the calculated minimum sample size was 216. The researcher visited the nursing department at each hospital to request participation, and to explain the purpose of this study and the contents of the questionnaires. A total of 250 questionnaires (120 and 130 questionnaires from the two hospitals) were returned, for a response rate of 95.2% (96.7% and 93.8% for the two hospitals); however, 19 questionnaires were incomplete or included inappropriate responses. Thus, 219 questionnaires were used in the final analysis.
3. Ethical Considerations
The study was approved by the K University Institutional Review Board of the researcher's institution (IRB; KNU 2016-0019), and performed in accordance with the declaration of Helsinki. To protect the participants' human rights, permission to collect data was obtained from the director of the relevant facility. Before the survey was administered, the purpose and process of the study, a guarantee of confidentiality, the condition of voluntary participation, anonymity of data, and the right to discontinue participation at any time during the process were explained to the participants. The written consent form clearly stated that participants could freely decide whether to participate in the study. The researcher informed participants that they could contact the researcher with any questions and could withdraw from the study at any time. For the protection of participants' personal information, the survey did not ask about information related to personal identity, and collected data were discarded when the study was finished.
4. Instruments
Each item in the three instruments was scored on a five-point Likert-type scale with responses ranging from 1 (strongly disagree) to 5 (strongly agree). Thus, higher scores indicated higher levels of TLB, OCB, and social capital of nurses.
5. Transformational Leader Behavior (TLB)
TLB was measured using the Multi-factor Leadership Questionnaire (MLQ), developed by Bass and Avolio [7] and evaluated for validity and reliability for use with nurses by Kim [1]. TLB indicates the staff nurses' perceived leadership related to the nurse managers' motivation skills, sharing of vision, and innovative capabilities in nursing care performance. It was used after obtaining permission via e-mail from Kim [1], who translated the MLQ. This instrument consists of 16 items categorized into three subscales: motivation skills (8 items), sharing vision (4 items), and innovative capabilities (4 items). The MLQ's Cronbach's α was .86 in Bass and Avolio [7], .90 in Kim [1], and .89 in the present study. The reliability coefficients of the subscales ranged from .76 to .85 in the present study.
6. Organizational Citizenship Behavior (OCB)
OCB was measured using the Organizational Citizenship Level Scale (OCLS) developed by Altuntaş and Baykal [3]. The OCB was translated into Korean in three steps. First the OCB was translated into Korean by two independent translators who are fluent in English, and by a Korean nurse. Second, three bilingual nursing faculty members, well-known in the area of nursing management, independently back-translated the Korean version into English. Then, a bilingual nursing faculty member evaluated the level of agreement between the original English version and the back translations on a scale of 0~10 (0=completely different, 10=almost identical). Each item from the three nursing faculty members' back-translations was evaluated and found to have an agreement score higher than eight points. Thirdly, the researcher compared the original and back-translated versions and agreed that there was consistency in meaning. Thus, the Korean translation of the OCLS was found to be valid. This instrument consists of 24 items categorized into five subscales: conscience (7 items), praising the institution (4 items), informing (5 items), tolerance (4 items), and helping (4 items). For the OCLS, Cronbach's α was .87 in Altuntaş and Baykal [3] and .88 in the present study. The reliability coefficients of the subscales ranged from .68 to .87 in the present study.
7. Social capital
Social capital was measured using the Social Capital Outcomes for Nurses (SCON) developed by Sheingold and Sheingold [17] and evaluated for validity and reliability for use with nurses by Shin and Lee [13]. It was used after obtaining permission via e-mail from Shin and Lee [13], who translated the SCON. This instrument consists of 36 items categorized into five subscales: internal trust and solidarity (12 items), external trust and solidarity (9 items), participation and empowerment (7 items), conflict (5 items), and social cohesion with coworkers (3 items). For the SCON, Cronbach's α was .92 in Sheingold and Sheingold [17] and .90 in the present study. The reliability coefficients of the subscales ranged from .75 to .88 in the present study.
8. Data analysis
The data were analyzed using SPSS/WIN 21.0. To describe the demographic characteristics of the study sample, descriptive statistics were calculated. To analyze differences in the level of OCB based on the participants' demographic characteristics, a t-test or an ANOVA and Scheffé's test were utilized. The levels of TLB, OCB, and social capital were analyzed using averages and standard deviations. Pearson correlation coefficients were used to examine the relationships among TLB, OCB, and social capital. To analyze the mediating effect of participant's social capital on the relationships between TLB and OCB, Baron and Kenny's [18] regression method was utilized. This method requires the following regression equations: the independent variable is a significant predictor of the mediator at Step 1; the independent variable is a signifi cant predictor of the dependent variable at Step 2; and the mediator is a significant predictor of the dependent variable at Step 3, although the effect of the independent variable must be greater at Step 2 than it is at Step 3. The Sobel test, used in the study of MacKinnon and colleagues [19], was also utilized to prove the influence of mediated effects in this study.
RESULTS
1. Demographic Characteristics
There was a total of 219 participants and 94.5% were female, with the highest proportion in their 20s (49.8%), followed by those in their 30s (30.1%) and 40s (20.1%). Regarding marital status, 64.4% of the participants were single and 35.6% were married. In terms of educational level, the greatest proportion had a bachelor's degree (60.3%) and a lower percentage had a 3-year college degree (31.1%). Regarding work experience, 37.0% of participants had practiced their profession for less than 5 years, approximately 47.0% had between 6 to 10 years' experience, and 16.0% had been practicing for more than 11 years. Regarding current department assignment, 87.7% of participants worked on a ward and 9.1% in an intensive care unit (Table 1).
2. Mean Scores among Measurement Variables
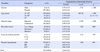
The participants' average TLB score was 3.13±0.46 points out of 5 points. The average for each subscale was 2.78±0.64 points for sharing vision, 3.26±0.73 points for motivation skills, and 2.80±0.68 points for innovative capabilities. The participants' average OCB score was 3.64±0.45 points out of 5 points. The average for each subscale was 3.83±0.50 points for informing, 3.39±0.62 points for praising the institution, 3.80±0.60 points for tolerance, 3.56±0.63 points for helping, and 3.62±0.58 points for conscience. The participants' average social capital score was 3.24±0.40 out of 5 points. The average for each subscale was 3.47±0.42 points for internal trust and solidarity, 3.28±0.55 points for external trust and solidarity, 3.03±0.54 points for participation and empowerment, 3.29±0.57 points for conflict, and 3.01±0.41 points for social cohesion with coworkers.
The absolute value for skewness of each of the variables was in the normal distribution, showing less than 1, and all absolute values for kurtosis were less than 3, satisfying the normal distribution requirements (Table 2).
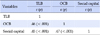
For the correlational analysis between the variables used in this study, an issue of multicollinearity can be raised if a correlation between the variables is more than .90; however, the largest correlation coefficient obtained in the analysis was .85. Therefore, no problem was observed regarding multicollinearity.
Statistically significant, positive correlations were found between TLB and OCB (r=.46, p<.001), TLB and social capital (r=.45, p<.001), and between social capital and OCB (r=.47, p<.001)(Table 3).
Mediating effect of social capital on the relationships between TLB and OCB.
According to the results of the regression analysis, the basic assumption of independence of the residual was satisfied by the Durbin-Watson test. The normality of the residual and the equal variance assumption were also satisfied. There were no issues revealed by testing for multiple collinearity among independent variables, as values for the Variance Inflation Factor (VIF) did not exceed 10.
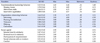
The results of our three-step regression analysis on the mediating effect of social capital on the relationships are shown in Table 4 and Figure 1. Based on the three-step regression method of Baron and Kenny (1986), we determined the mediating effect of social capital on the relationship between TLB and OCB. In step 1, TLB (independent variable) had a significant effect (β=.39, p<.001) on social capital (mediating variable). In step 2, TLB had a significant effect (β=.61, p<.001) on OCB (dependent variable). Lastly, a model that considered both TLB, as an independent variable, and social capital, as the mediator, revealed that social capital had a statistically significant positive impact on OCB (β=.16, p<.001). The model also indicated that the β value for TLB stress equaled .16, which was lower than the β value from the second analysis (.61). Furthermore, this model highlighted the statistically significant impact of TLB on OCB (p<.001). Therefore, the results suggest that social capital plays a partial mediating role in the relationship between TLB and OCB. The results of the Sobel test indicated a significant mediating effect with z=6.63 (p<.001).
DISCUSSION
This research was conducted to demonstrate the importance of social capital by investigating its mediating role in the relationship between TLB and OCB, and to provide fundamental information for the development of a nursing workforce management plan, which is essential in improving OCB.
The levels of TLB reported by nurses in this study were somewhat lower than the mean score obtained from 200 nursing staff, i.e., nurses and medical assistants [20]. According to the results of this study, the highest TLB subscale scores were for motivation skills, while sharing vision was lowest. There are various organizational personnel in hospitals, so it may be difficult for nurse managers to exert their leadership and increase motivation towards a common goal. TLB helps to motivate organization members to achieve outcomes beyond personal interests and to recognize the value of their work [2122]. Nurse managers, therefore, need to provide sensitive attention and instill persistent beliefs in order to help staff nurses to have confidence in their nursing practice. Through organic relationships between leaders and staff, TLB enables leaders to present a vision to organization members and to help motivate them to achieve innovative goals [1]. Smith [6] reported that ‘sharing vision’ had effective in achieving greater organizational performance by encouraging members to pursue their common goal. But the sharing vision of hospital organization was lacking in this study. Therefore, nurse managers need to provide leadership that share their vision with their staff nurses to achieve broad goals for all hospitals, beyond their personal interests.
The level of OCB (72.8 converted to 100 points) in this study was similar to the result (72.1 converted to 100 points) obtained in the study by Cavanagh and colleagues [23], which was conducted among nurses in an Australian hospital. However, the study result was lower than that (80.3 converted to 100 points) of the employees in the study conducted by Amintojjar and colleagues [5]. According to the results of this study, the OCB subscale scores were highest for conscience and lowest for praising the institution. Conscience is the willingness of organization members to display behaviors beyond the minimum role behavior expected from them [3]. Praising the institution comprises the active participation of workers in the political life of the organization [3]. For instance, it includes some behaviors such as regularly attending intra-organizational meetings and discussions, closely following changes in the organization and offering solutions to problems, and joining in decisions made within the organization. Due to the nature of hospitals, which deal with life, OCB is a major factor in nurses' helpful behaviors that include helping their clients voluntarily and preventing occurrence of work-related problems. Health-care organizations are workforce intensive, where the need for staff or human resources cannot be replaced with technology. Moreover, they are faced with high levels of attrition due to work stress and a mismatch between demand and the supply of talented professionals [24]. Hence, they have to constantly face a challenge of staff shortages in running day to day operations. In such a context, it is important that nurse managers acknowledge the concept of OCB and attempt to identify, attract, and retain those nurses capable of exhibiting such behaviors for organizational functioning and effectiveness.
The level of social capital (64.8 converted to 100 points) in this study was similar to the result (64.4 converted to 100 points) obtained in the study by Jang and colleagues [25], which was conducted among hospital nurses. However, the levels were higher than those reported (45.0 converted to 100 points) in research targeting adult workers in various sectors [26]. Collectively, nurses appear to have higher social capital levels than do individuals in other occupations. Social capital refers to intangible assets that arise from social relationships that increase organizational productivity, such as internal and external trust and solidarity, participation and empowerment, conflict, and social cohesion with coworkers. According to the results of this study, social capital scores were highest for the internal trust and solidarity subscale and lowest for social cohesion with coworkers. Sheigngold and colleagues [2] found that elements of social capital, such as trust and participation in civic activities, were positively related to organizational performance. According to Cavanagh and colleagues [23], social capital, as the sum of the internal and external trust derived from the network of relationships possessed by a social unit, had a strong effect on nurses' OCB. Thus, nurse managers should seek to develop a structure and create processes to build mutual trust with other nurses, healthcare professionals, or people in different positions. Social capital based on shared trust improves nurses' capacity to share solidarity and participation through their networks to accomplish organizational goals. Finally, they will be able to cooperate in their assigned nursing practice tasks, follow the instructions of managers, and respect the rules of professional nursing practice.
According to the correlations between TLB, OCB, and social capital, both the TLB and social capital of nurses showed a significant positive correlation with OCB. These findings are consistent with the previous study by Jha [12], who examined the relationship between TLB and OCB in employees of five-star hotels. Nurses who are the most active members of the health-care staff should display high levels of OCB in order to more efficiently provide health services [3]. Through a better work environment that increases nurse managers' TLB to achieve their goals, it is possible to increase their OCB by enhancing social relationships among hospital workers. In studies conducted to determine the relationship between social capital and OCB [527], positive relationships were found to exist between these two variables. In a study conducted by Jha [12] with 319 hotel employees, a significant and positive relationship was found between transformational leadership and OCB. Asgari and colleagues [4] similarly reported that the leader-member exchange was influential on staff's OCB.
It was confirmed that nurses' social capital showed a partial mediating effect in the relationship between TLB and OCB. Adding the positive transformational leadership of nurse managers has a direct corresponding effect on OCB; the positive transformational leadership of nurse managers also increases the level of nurses' social capital. That is, a nurse managers' positive transformational leadership may contribute to enhancing OCB. Concurrently, nurses with high social capital in their roles will endeavor to perform their full duties with mutual trust and embody the desirable aspects, such as a sense of empowerment and social cohesion with coworkers [15]. They are also likely to know how to co-operate with their health care teams who have to produce effective work to achieve high-quality patient care [13].
The results clearly suggest that social capital should be including in the development of training programs to enhance the OCB in health-care settings. The results also support the previous findings that the social capital of volunteer in human services was the mediation effect in relationship between citizen participation and volunteer activity [28]. This finding is also in line with a study indicating that nurse managers must try to enhance nurses' social capital, which is accessed via the organization's culture based on shared values, beliefs, and trust. Recently, as concern about organizational change though social capital has increased, health-care services emphasizing individual social responsibility are also gaining importance [2]. The main factor affecting the OCB of hospital nurses is their attitudes toward the organization, and these attitudes can be affected by social capital [25]. Social capital refers to the actual and potential resources that can be obtained through social relationships within a particular organization's social structure [2]. The findings of this study highlight the importance of social capital that provides opportunities for active participation in organizational affairs and empowers nurses to accomplish their nursing work. Social capital cultivates OCB, which enhances work motivation by enhancing a sense of unity and facilitating member activities [29]. It will also be helpful to develop a program to strengthen social capital which reflects the unique organizational environment, in order to promote OCB.
CONCLUSION
These findings showed a partial mediating effect of social capital in the relationship between TLB and OCB. The findings are significant with regard to the importance of social capital in workforce management strategies to enhance nurses' OCB and suggest that social capital should be treated as an important predictor of OCB. However, the nature of this study's sample in the South Korean private sector is considered a limitation. Owing to this, the national and leadership cultures in which the participants of this study were affiliated may differ from previous studies. Thus, more cross-cultural and national comparison research using systematic sampling strategies is recommended. Moreover, any generalized interpretation of the findings of the study to other settings should proceed with caution.
More research is needed to investigate the causal relationship and to explore the application and effects of social capital in enhancing nurses' OCB so as to produce concrete evidence for incorporating social capital into nursing workforce management plans.


 XML Download
XML Download