

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Today’s hospitals have difficulties with high turnover among nurses, and a major reason of nurse turnover is job stress [1]. Turnover intention is an employee's intent to find a new job with another employer. Turnover intention used measure of turnover, because turnover cannot be measured actually [2]. Job satisfaction is a pleasurable or positive emotional state resulting from the person's job or job experiences. High job satisfaction is associated with low employee turnover [12]. Job stress is defined as feelings of anxiety, conflict, and pressure from various conditions that affect job satisfaction and organizational commitment negatively and increase absenteeism and turnover [23]. Individuals who experience stress chronically may have ineffective coping strategies for treating their emotional and physical pain with defensive or avoidance strategies. Such individuals may become apathetic, cynical, angry, or depressed [45]. Higher job stress is related to higher compassion fatigue [3].
Compassion fatigue is a prevalent phenomenon in the field of nursing. Joinson [4] first used the term compassion fatigue to describe the prevalent experience among professional caregivers such as nurses, physicians, and mental health counselors. The results of compassion fatigue are physical, emotional, social and psychological maladaptation, burnout, grief, depression, sleeping disturbance, and confusion etc.[4]. It is caused by prolonged, continuous, and intense contact with patients and exposure to stress [6]. Compassion fatigue puts nurses at high risk for poor professional judgment and incorrect assessments [78]. In addition, compassion fatigue accompanies reduced job satisfaction and increased turnover [3].
Thus, in-depth research on compassion fatigue needs to be conducted. In a previous study of post-traumatic stress and coping in 69 nurses, study participants with lower levels of coping had higher levels of post-traumatic stress [9]. Social support can enhance resilience to stress and decrease the functional consequences of trauma-induced disorders, such as post-traumatic stress disorder [10]. Indeed, perceived social support has a positive effect on the nursing work environment [11]. Coping is expending conscious effort to solve personal and interpersonal problems, and seeking to minimize stress. Thus, coping skills and social support are influential factors regarding compassion fatigue, job satisfaction, and turnover [31213]. Much research has addressed the relationship among job satisfaction, organization commitment and turnover intention in nurses. There are few studies on how compassion fatigue, coping, social support affect job satisfaction or turnover intention in nurses. Therefore, the aim of this research was to identify the important factors of turnover intention considering compassion fatigue, coping, social support, and job satisfaction in clinical nurses. The results of this study should contribute to management strategies for retention of hospital nurses.
1. Research Purpose
For this study a path analysis was done of turnover intention, compassion fatigue, job satisfaction, coping, social support in clinical nurses who had worked in emergency room, intensive care unit, pediatric unit, psychiatric unit, or oncology unit. The aims of this research were to construct and verify a model of turnover intention in clinical nurses, considering compassion fatigue, coping, social support, and job satisfaction.
MATERIALS AND METHODS
1. Design
We used a cross-sectional correlational design to construct and verify a model of turnover intention among clinical nurses. The conceptual model was constructed with information from a literature review of studies [2361113]. The literature review revealed that nurses' age and career, workload, and experience of trauma events affected compassion fatigue. Social support and coping mechanisms also affected compassion fatigue, which in turn affected job satisfaction and turnover intention. The basic theories of this research are based on Figley's compassion fatigue process [3], and Price and Muller's causal model of turnover [14], which included relationships among job stress, social support, job satisfaction, and turnover intention, as well as Mobley's intermediate linkages model [15], which included relationships among demographic factors, work environment, job satisfaction, and turnover intention.
2. Setting and Samples
The targets were clinical nurses working at four tertiary hospitals in Korea. Using a convenience sampling method, 330 clinical nurses were recruited for the research from the psychiatric ward, oncology ward, pediatric ward, an emergency department or intensive care unit. According to a literature review [13], nurses working these units reported higher compassion fatigue.
The inclusion criteria for participants were (a) currently working full-time for longer than 1 year (b) currently participating in direct patient care; and (c) able to respond to a questionnaire. The final sample was 283. The formula for sample size in path analysis is 1.5 × Q (Q+1), where Q is the number of observed variables [16]. Because 13 variables were used in this research, 273 nurses would be required. Thus, the sample size was adequate for the research.
3. Ethical considerations
Prior to collecting data, we received approval from the Institutional Review Board (IRB) of the university with which we are affiliated (DKUH 2012-10-005-001). This approval covered collecting data from the four hospitals. In addition, we explained the purpose of the study to all participating nurses and secured their written agreement to participate. We also explained that they could withdraw from participating in the data collection without any penalty.
4. Instruments
1) Personal and work characteristics
Personal characteristics included gender, age, marital status, educational background, religion, career, clinical setting, and workload.
2) Occupational trauma events
The tool used to measure occupational trauma events consisted of 16 items, constructed on the basis of a review of the literature [917]. The Cronbach's α was .82. For 16 types of occupational trauma events, ‘0’ was coded for no experience and ‘1’ for experienced. The reliability of occupational trauma events was analyzed by using KR (Kuder Richardson)-20 method.
3) Coping
Coping was measured using Yang's tool [18], which consists of 13 items for problem-focused coping and 17 for emotion-focused coping rated on a five-point Likert scale; this tool was adapted from Lazarus and Folkman's Way of Coping Questionnaire [5]. In this research, the Cronbach's α was .86 for problem-focused coping and .85 for emotion-focused coping.
4) Social support
Social support is what people perceive as care and love from other people. Park's tool [19] for measuring social support relies on 25 questions rated on a five-point Likert scale. In the present study, scores for support from family and from friends were combined into family-friend support, which had a Cronbach's α of .99.
5) Compassion fatigue
Compassion fatigue was measured using one subscale for ‘compassion fatigue/secondary traumatic stress’ from the Korean version of the Professional Quality of Life Scale (ProQOL) developed by Stamm [20]. ProQOL is structured as a 30-item scale with three subscales. In the present research, Cronbach's α was .86.
5. Data collection
After receiving IRB approval., we first contacted nurse managers who were in charge of nursing departments via telephone. We tried to avoid selection bias in the target hospitals, so we collected data at four general hospitals from three regions in Korea with 800 beds and similar characteristics. The participants were asked to seal the self- reported questionnaires and put the box, and then the nurse managers collected and sent them to the researchers by mail.
RESULTS
1. General Characteristics of Participants
The general characteristics of participants are shown in Table 1. The mean age was 30 years. Most participants were female nurses (n=274, 96.8%), and more than half were single (n=179, 63.3%). Nurses with a bachelor's degree numbered 142 (50.2%), and 146 nurses did not specify a religion (51.6%). Nurses total career data were as follows: under three years, 81 (28.6%); three to five years, 68 (24.0%); five to 10 years, 84 (29.7%); and longer than 10 years, 50 (17.7%). Emergency room nurses numbered 52 (18.4%), intensive care unit nurses 102 (36.0%), pediatric unit nurses 46 (16.3%), oncology unit nurses 53 (18.7%), and psychiatric unit nurses 30 (10.6%). The majority of the nurses responded that their workload was ‘overload’ (n= 175, 61.8%).
2. Descriptive Statistics of Research Variables
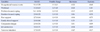
The means of the variables except the variable ‘family-friend support’ were higher than the middle scores of their tools. The ranges of skewness and kurtosis of the research variables were less than ±3 (Table 2). The correlation coefficients of research variables ranged from .05 to .63. Because the data distributions were appropriate and highly correlated variables were not shown, the data were suitable to testing the model.
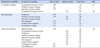
The details of experiences of occupational trauma events are shown in Table 3. Only four participants (1.4%) responded that they did not experience any occupational trauma event. The rest (98.6%) revealed the experience of at least one occupational trauma event during their clinical career. The highest experience was verbal or behavior violence of patient or patient's family (n=261, 92.2%). It was also revealed that more than half of nurses experienced occupational trauma events for variables, such as patient's suffering status (n=236, 83.4%), inconsiderate attitude of medical staff to patients (n=222, 78.4%), grief of patients' family (n=221, 78.1%), patients' death (elderly)(n=207, 73.1 %), verbal or behavioral violence of doctors (n=197, 69.6%), their peers' big mistake on the job (n=178, 62.9%), failure of patients' CPR (n=173, 61.1%), doctors' big mistake on the job (n=172, 60.8%), my big mistakes on the job (n=168, 59.4%).
3. Test of the Model
1) Hypothetical Model
The fit of the hypothesis model was GFI=0.96, NFI=0.88, CFI=0.88, and RMSEA=0.16. The values of NFI, CFI and RMSEA showed a low level of acceptability. Acceptable value of GFI, NFI, and CFI is over .9, and acceptable value of RMSEA is .06 to .08. The hypothetical model was revised considering theory justification and using the critical ratio and the modification index from the path analysis results. Among 19 paths in the hypothetical model, 11 insignificant paths were deleted and 2 were added. Finally the model was modified with 10 paths.
2) Modified Model
The test of the modified model demonstrated a good fit (GFI=.98, NFI=.95, CFI=.96, and RMSEA=.07), which was more parsimonious than the hypothetical model (Figure 1).
Compassion fatigue had three significant paths from occupational trauma events (β=.18, p<.01), from problem-focused coping (β=−.14, p<.05), and from emotion-focused coping (β=.47, p<.01). These variables explained 21% of the variance for compassion fatigue. Job satisfaction had four significant paths from workload (β=−.33, p<.01), from problem-focused coping (β=.17, p<.01), from peer support (β=−.37, p<.01), from family-friend support (β=.15, p<.05) and from compassion fatigue (β=−.11, p<.05). These variables explained 29% of job satisfaction. Turnover intention had two significant paths from marital status (β=−.12, p<.01) and from job satisfaction (β=−.61, p<.01). These variables explained 40% of the turnover intention (Table 4).
DISCUSSION
The aim of this research was to identify the important factors of turnover intention as related to compassion fatigue, coping, social support, and job satisfaction in clinical nurses. We tested the model of turnover intention, considering compassion fatigue, job satisfaction, coping, and social support in clinical nurses working more than 1 year on psychiatric wards oncology wards, pediatric wards, emergency departments or intensive care units. These clinical departments were selected based on review articles that reported that nurses working in these places had higher levels of compassion fatigue [1325].
In the modified model, we found that occupational trauma events had a positive direct impact on compassion fatigue. Several previous studies have also reported that higher occupational trauma events are correlated with higher compassion fatigue [1226]. In our result, it was found that the most common occupational trauma event was verbal and behavioral violence from patients. Buurman et al.,[9] found that physical aggression (86.6%) was the most frequently cited cause of traumatic stress. Niiyama et al.,[17] reported that the major trauma experience was violent language by a physician, or supervisor. These results indicate that the verbal abuse in the nursing workplace is a widespread phenomenon and controlling it could be an effective strategy for lowering compassion fatigue.
In the results, emotion-focused coping was the strongest factor influencing compassion fatigue and, problem-focused coping and emotion-focused coping affected compassion fatigue in the opposite direction. That is, nurses using emotion-focused coping more often could feel more compassion fatigue than those using problem-focused coping. These results indicate that education and training in problem-focused coping skills would be effective to overcome compassion fatigue for nurses in the workplace.
Job satisfaction explained 29% of the variance, directly by workload, peer support and compassion fatigue negatively, and problem-focused coping and family-friend support positively. In our participants, a heavier workload did not affect compassion fatigue but had a direct effect on decreased job satisfaction. In addition, the path direction from peer support to job satisfaction was contrary to our expectations. In other words, nurses having more peer support showed less job satisfaction. Maybe the nurses who had more peer support might have difficulties in doing their work, so eventually their job dissatisfaction grows. However, further research is needed to investigate this phenomenon. In this result, compassion fatigue negatively affected job satisfaction and problem-focused coping affected it. These results were consistent with previous studies [1217]. The level of turnover intention in our participants was above the medium (3.7 of 5). This score was higher than that of a previous study. Sung et al. [3] reported that the average score of turnover intention was 13.9 of 30. This difference might be due to the target population. In this study we controlled the participants' clinical departments, but in the study of Sung et al., all departments of tertiary hospital were included.
Turnover intention was directly affected by marital status and job satisfaction. Job satisfaction was revealed to be the most important variable of turnover intention. This result was consistent with previous research. Yang [27] also reported that job satisfaction was revealed as an important factor of turnover in nurses working in intensive care units. In our result, married nurses had lower turnover intentions than unmarried nurses. That is, if a nurse was a married nurse, she would have less turnover intention even though she was unsatisfied with her job. In other words, marriage could be a major independent factor affecting intention decisions.
Compassion fatigue was not a significant factor affecting turnover intention neither directly nor indirectly. However, Sung et al. [3] showed that compassion fatigue was a significant variable affecting turnover intention in nurses working on general wards. The difference compared to our research was the research settings. There is a need to conduct further research in that the uncontrolled research settings could bring about a different result.
In this study, we demonstrated and validated the empirical relationships among nurses' job satisfaction, turnover intention, and compassion fatigue. Also we found that coping is more related to compassion fatigue and social support is more related to job satisfaction. The modified model of turnover intention had a good fit in this study. Job satisfaction was the most important factor for controlling turnover intention. Job satisfaction was affected by workload, problem-focused coping, peer support, family-friend support and compassion fatigue. Nurse manager have to consider nurses' workload, coping, support, and compassion fatigue to maintain proper circumstances for nursing. In addition, hospital and nursing department should consider policy about managing the compassion fatigue and job satisfaction of nurses to increase retention.
CONCLUSION
We examined the factors affecting turnover intention, considering compassion fatigue, coping, social support, and job satisfaction in clinical nurses. Our participants reported a medium-high level of turnover intention, which was affected by job satisfaction and marital status. Job satisfaction was affected by workload, problem-focused coping, peer and family/friend support, and compassion fatigue. Compassion fatigue was affected by occupational trauma events; it was positively affected by problem-focused coping and negatively affected by emotion-focused coping. Nurses have to learn how to manage compassion fatigue. They also need to develop problem-focused coping skills and should receive support to achieve job satisfaction. In addition, nurse managers should establish a reasonable workload for nurses, and nurses have to be aware of the relationship between occupational trauma events and compassion fatigue. These efforts can increase the rate of job satisfaction and care quality of nursing departments. There is a limitation in interpretation of this study, because of analyzing data of several departments in some hospitals.



 XML Download
XML Download