

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
As nurses have more incentives to improve their career and clinical nursing knowledge, there are more and more nurses pursuing further nursing education. Recently, more registered nurses (RNs) with diploma or associate degrees are attending RN-BSN programs. At an international nursing conference in Korea, it was reported that because of the popularity of certified nurse specialist, the number of nurses who want to continue post-graduate nursing education was increasing (Horiuchi, 2009). As nurse pursue further education while they are working, they assume the additional role of student, as well as the roles of worker.
The role expectations of women and men in Asian society are different (Kim, Baik, & Kim, 2002). Compared with men, women are expected to assume multiple roles;consequently they have more role-related stress. Nurses, most of whom are women, as professional individuals, hold at least two roles or more that of home maker and as an employee in an organization. For men the significant role is as a worker, especially in Asian countries.
Inter-role conflict occurs when an individual occupies two or more roles whose expectations are inconsistent. Based on Kahn et al.'s (1964) conceptualization of role conflict, in the present study, interrole conflict occurs when pressures from the work, family, and/or school domains are mutually incompatible, including work and school interfering with family, (WSIF), family and school interfering with work (FSIW), and family and work interfering with school (FWIS).
In many studies on role-related stress in nurses (Lambert & Lambert, 2001), the focus of the studies was on identifying stressors in the work environment. Killien's literature review study (2004) reported that factors of work-family conflicts significantly affect job stress, and that work and family responsibilities have a significant relationship with home stress among women workers. According to Neuman's system model, work-family conflict, a type of interrole conflict' is an intrapersonal stressor occurring within the individual (Tomy & Alligood, 2001).
Stress has been widely implicated as a factor in the development of health problems for men and women, and especially for professional workers (Houle, 2003). In one study on stressful life events among college women, it was reported that the participants experience high level stress, a dangerous risk factor for depression (Kim & Oh, 1999).
Nursing is a highly stressful occupation, and high levels of occupational stress are believed to affect the physical and mental health of nurses (Wu et al., 2010). The effects of acute and chronic stress are a major concern to nurses (Corey et al., 1999). One type of stress frequently studied among employed women is role-related stress. Role-related stress has been defined as the consequence of a disparity between what an individual perceives as expectations of a certain role and what the person actually accomplishes in that role (Lambert & Lambert, 2001).
Recently, the potential interrole conflict in nurses has become a concern for nursing management, because it generates many negative consequences, such as low job satisfaction, job turnover, high stress, and poor health for the professional employees (Gipson-Jones, 2009; van der Heijden et al., 2008). Interrole conflict is a problem of particular importance to RNs pursuing further studies, as the nurses must maintain work and/or family responsibilities in addition to those related to school.
METHODS
Research design
We used a correlative research design in this study, with self-administered questionnaires.
Sample and procedure
The target population was Korean female registered nurses who were pursuing studies in advanced nursing education programs, drawn from the nursing programs of 4 universities in D city, Korea. RNs in RN-BSN programs and RNs pursuing master or doctoral nursing degrees were included in the study and all of them assumed two or more roles. Convenience sampling was used to obtain the sample of 149 RNs, including RNs in RN-BSN programs (65.1%) and RNs pursuing master or doctoral nursing degree (34.9%). As there were few studies on the work-family-school conflict, according to the convention for power analysis, we used a medium effect size of size of 0.15 for the regression analysis, the significance level of 0.05, a power of 0.80, and 8 predictors. After calculating, a sample size of 109 was found to be necessary (Cohen, 1988).
For data collection questionnaires packages were given to the participants by the study researchers. Before sending the questionnaire packages IRB approval was received from the university where researcher B is affiliated. The package consisted of a self-administrated questionnaire and a cover letter specifying the purpose of the survey and the voluntary nature of participation, and emphasizing the confidentiality of responses. Of the 200 questionnaires distributed, 149 were returned with an effective response rate of 74.5%.
Measurement
Questionnaires were in Korean, but were initially constructed in English and then translated into Korean by researchers who are native Korean and good at English. To validate the Korean version, another professional nursing doctoral student was asked to back-translate the questionnaire into English.
Interrole conflict
In previous nursing studies, interrole conflict was frequently measured with 10 items developed by Netemeyer, Boles, and McMurrian (1996) which measured work-family conflict including two parts, work interfering with family and family interfering with work (van der Heijden et al., 2008; Simon et al., 2004). Netemeyer et al. (1996) provided evidence for the scale's construct validity and reliability. They reported an average reliability of .88 for work to family conflict and .86 for family to work conflict across samples.
In this study, based on Netemeyer et al.'s (1996) scale, we adapted a 15-item scale to measure the interroleconflicts among the registered nurses pursuing advanced study, including three sub-scales, work and school interfering with family (WSIF), family and school interfering with work (FSIW), and work and family interfering with school (WFIS). Response options ranged from strongly disagree (1) to strongly agree (5). The Korean version reliability for the WSIF scale was .93 for the sample, FSIW was .90, and for WFIS, .94.
Role-related stress
In this study, the three kinds of role-related stress (family stress, work stress, and school stress) were assessed by monthly Numeric Rating Scales (NRS): 0-10.
Data analysis
The data were analyzed using the SPSS WIN v. 18.0 program. Frequencies, percentages, means, and standard deviations were calculated to summarize the descriptive data. Pearson's correlation coefficients were calculated to examine the relationships between studied variables. Multiple regressions were used to furthertest the relationships among interrole conflicts and perceived role-related stresses among the registered nurses pursuing nursing degrees. Prior to the regression analysis, homoscedasticity, independent errors (Durbin-Watson test) and multicollinearity with tolerance values were tested. In the hierarchical multiple regression model for role-related stress, among the demographic variables work position which was significantly related with role-related stress was entered first, and the interrole conflict variables were entered in the second step.
RESUSLTS
Demographic characteristics of the participants
Of the participants, 57% (n=85) were under 30 years of age, and 12% (n=18) were over 40. For type of study program, 65% (n=97) were enrolled in RN-BSN programs and 35% (n=52) in nursing master or doctoral programs. The majority of the participants were staff nurses (n=128), but 14% worked as head nurses or nursing manager (n=21). Regarding clinical experience, about 50% had worked in a hospital for less than 5 years (n=75), and 19% (n=28) had worked more than 10 years. Participants reporting (n=101,) duty on all three shifts, including day shifts, evening shifts and nigh shifts accounted for 69% of the participants. The remainder only worked on the day shift (n=46). Participants who were married (n=41) made up 28% of the sample, and 23% of the participants stated that they had children (n=34). The number of children ranged from one to three. Further, 24% reported having family members with chronic diseases(n=36), (their spouses, children, and/or parents) <Table 1>.
Descriptive statistics of interrole conflict and role-related stress among the participants
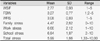
Table 2 shows means and standard deviations for the interrole conflict variables and perceived role-related stress of the participants. Work-school interfering with family conflict had the lowest score with a mean value of 2.77 (SD=0.93), Family-school interfering with work had the highest score with a mean of 3.27 (SD=0.77), and Family-work interferingwith school was at the mid level (Mean=2.92, SD=0.83). Interrole conflicts for the participants were in the moderately high levels. Family stress had a mean of 4.47 (SD=2.62), work stress, a mean of 6.66 (SD=2.12), and school stress, 6.84 (SD=1.87). The mean for total perceived role-related stress was 5.99 (SD=1.66). For the NRS with role-related stress scores ranging from 0 to 10, high scores indicated high level stress. In this study family-related perceived stress was at the mid level, and work stress and school stress were slightly above the midpoint <Table 2>.
Differences in role-related stress by demographic characteristics
For the demographic characteristics, only work position had a significant relationship with role related stress (t=-1.99, p=.048), and head nurses or nursing managers (Mean= 6.69, SD= 2.21) had significantly more stress than staff nurses (Mean= 5.93, SD=1.66) <Table 3>.
Relationships of work position, interrole conflict and role-related stress
Table 4 shows the relationships between interrole conflicts and role-related stresses. Work position had a significant relationship with role-related stress, and all the relationships between interrole conflicts and role-related stresses were significant, ranging from .23 to .38, with the exception of the relationship of FWIS and family stress <Table 4>.
Predictability of interrole conflict on role-related stress in multiple linear regressions
Table 5 presents the empirical findings of multiple regression analysis on perceived role-related stress. As shown in the Table, model 1 with the predictor or work position (staff nurse =1) contributed significantly to role-related perceived stress (F=3.97, p=.048), explaining 2% of the variance of total role related stress. After adding the interrole conflict variables (WSIF, FSIW, and FWIS), model 2 was significant in accounting for 23% of the variance of total role-related stress. In the model, work-school interfering with family (β =.34, p<.001) was the first important predictor significantly contributing to role-related stress, family-school interfering with work (β=.17, p=.049) was the second important predictor significantly contributing to perceived role-related stress, and family-work interfering with school was not significant <Table5>.
DISCUSSION
Findings from this study provide a basis for the perceived relationship between interrole conflict and role-related perceived stresses, and whether interrole conflicts predict role-related stress for RNs pursuing further nursing education.
According to our results on interrole conflicts, the participants had the highest score for family-school interfering with work, and the lowest score for work-school interfering with family. This finding indicates that compared to family and school demands, the participants cannot prioritized work demands. Returning to school was a challenging act for nurses, as they were struggling with family, work, school and personal goals (Kalmanet al., 2009). These findings were not consistent with a previous studyabout nurses in RN-BSN program in which the participants usually prioritized family and work over school demands (Kalmanet al., 2009). In the present study, for perceived role-related stresses, school stress had the highest level (Mean=6.84, SD=1.87), andthe total role-related stress was higher than the mid-level. About half of the participants had worked for more than 5 years, and they had been out of school for many years. Consequently, when they returned to school for advanced nursing degrees, they experienced more school stress due to work and family commitments (Delaney & Piscopo, 2004).
In the present study, for differences in role-related stress according to demographic characteristics, only work position was significantly associated with role-related stress.
The results for age, education and clinical experience were not consistent with previous studies (Grzywacz et al., 2006; Hamaideh, 2011; Kirby, et al., 2004) which reported that age, greater education, and clinical experience were positively related with stress and family stress. Having religion was not correlated with perceived role-related stress, and this was not consistent with a previous study (Mann et al., 2010) in which religiousness/spirituality was negatively associated with perceived stress for women. Previously, Fujimoto et al., (2008) reported that shift work with nights was positively related with interrole conflict and role-related stress, but the results of the present study do not support this finding.
In previous studies (Grzywacz et al., 2006; Yildirim & Aycan, 2008) it was reported that the RNs who were married and were parents with children living at home had greater stress than those who did not, but this finding was not supported in the present study. In the present study, while 72% of the participants were married, only 23% had children. Therefore in the future studies, there is a need to include more married participantsto further examine the relationships demographic characteristics and role-related stress.
For the variable of having family members with chronic disease, the findings were not consistent with previous studies which reported that family members (adult children, spouse, and parents) even with chronic disease were supportive of return to school. This support could decrease stress, and improve psychological well-being in the nurses (Chen et al., 2007; Gipson-Jones, 2009; Kalmanet al., 2009; Mann et al., 2010).
Regarding the correlation between work position and perceived role related stresses, the results are similar to findings of previous studies (Camerino et al.,2010;Yildirim, 2008), that staff nurses had significantly lower levels of family stress compared to head nurses or nurse managers. In the present study, most of the participants were single (72.3%), and most were staff nurses. The interrelationships among the variables should be tested in the future, to determine whether the lack of a relationship between most of the demographic characteristics and the total role-related stress can be explained.
For the influence of interrole conflicts on role-related stress, our findings revealed that WSIF and FSIW were significant predictors to role related stress. Work-school interfering with family was significantly related to role-related stress which is consistent with prior studies among nurses in college, that the interference with their family life by work and study caused them to feel stressed and anxious and to have lower levels of life satisfaction (Gipson-Jones, 2009; Yildirim & Aycan, 2008).Widespread work-family conflict is a concern in light of previous research indicating that work-to-family conflict and family-to-work conflict contribute to decreased job satisfaction (Adamet al., 2009, Chen et al., 2010), stress (Stephens et al., 2001), and health problems (Burke & Greenglass, 2001) among females. The findings showing WSIF and FSIW influences role-related stress are supported by previous studies. WFIS was not a significant predictor of role-related stress which was not consistent with a previous study about work-school conflict among college students (Butler, 2007).
To better understand the predictors of role-related stresses and the factors influencing interole conflict among nurses pursuing further education, in addition to the variables in the family domain and work domain examined in this study, in the future research should be done with other relevant variables, including work overload in the job (Chen et al., 2007; Limet al., 2010; Admi, & Moshe-Eilon, 2010), social support, and also some school domain variables of long study hours, and distance education programs (Gipson-Jones, 2009; Kalmanet al., 2009).
This study has several limitations which provide opportunities for future research. First no attention was given to the variables in school domains and variable of social support. Social support (Hamaideh, 2011) and the school domain variables (Bulter, 2007), such as studying hours, were found to influence the levels interrole conflict and role-related stresses. Second, in studying the interrole conflict, it is necessary to include more RNs who are married and have preschool children. It was reported that this population has higher levels of interrole conflict and stress (Fujimoto et al., 2008). Third, to analyze the complex relationships among the interrole conflict variables and include more related variables, construction of a structural equation model is recommended. Finally, the data in the study were collected in one city only limiting the generalizability of the findings.
CONCLUSIONS
Results from this study indicate that there are perceived relationships between interroleconflict (WSIF, FSIW, and WFIS) and role-related stresses (family stress, work stress, and school stress) among the increasingly large group of nurses pursuing further nursing education, especially in Asia where women are the main homemakers in the family. The study has the potential to contribute to the research literature as well as nursing practice by identifying the predictors of role-related stress among the RNs pursuing further nursing education degrees. The findings point to the necessity of redesigning the work conditions of RNs who are in education programs and possibly limit night shifts to reduce interrole conflict. In order to encourage more and more RNs to continue further nursing education and to increase their nursing knowledge and skills, the nursing administration department should provide some rewards or make preferential policies, or rules to decrease their role-related stress, and the supervisors should increase their empathy and assistance in handling the interrole conflict problems of this group of nurses.



 XML Download
XML Download