

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Folate, initially investigated as an antianemia factor, has a major role in one-carbon transfer reactions in the biosynthesis of nucleic acids and metabolism of amino acids. In recent years, much attention has been given to folate due to its potential roles in preventing neural tube defects (NTDs), cardiovascular diseases and certain types of cancer [1-3]. In addition, folate may have other crucial roles in cognitive function and bone health [4,5]. Therefore, adequate folate nutritional status throughout all stages of life is considered to be important for health maintenance and chronic disease prevention.
Folate nutritional status of a given population is usually assessed by measurement of folate concentrations in the serum/plasma or red blood cells (RBCs). Serum folate is known to be a good indicator of recent folate intake, and RBC folate is a long-term indicator of folate status. Folate concentrations of less than 3 ng/mL in serum and less than 120 ng/mL (or 140 ng/mL) in RBC were traditionally considered as inadequate folate status [6,7]. The greatest reduction in NTDs, however, was observed at serum concentrations greater than 7 ng/mL compared to those of less than 3 ng/mL or RBC folate concentrations greater than 400 ng/mL compared to those of less than 150 ng/mL in pregnant women [8], suggesting that desirable range for blood folate in women of childbearing age may need to be changed in order to reduce the incidence of NTDs.
College years are a period when most students start to live relatively freely from their parents. Most of them do not depend on regular meals at home anymore and may have to decide what to eat for each meal. The decisions they make in their twenties may influence health later in life [9]. However, inadequate nutrient intakes and poor dietary habits, as well as unhealthy behaviors, such as smoking and alcohol drinking among college students, have been reported [9-11]. When dietary intakes of Korean college students were compared in 1999 and 2009, intakes of energy and most other components including fat and cholesterol were significantly higher in 2009 compared to 1999, but intakes of vitamin C and folate were similar and dietary fiber intake was significantly lower [11], indicating that their intakes of fruits and vegetables have been decreased over time. Chen et al. [12] showed that the mean serum folate concentrations were the lowest and the prevalence of folate deficiency and insufficiency was the highest in both men and women aged 19-30 years compared to other age groups older than 31 years. In addition, they showed that young adults aged 19-30 years consumed dark green vegetables and fruits least frequently among all age groups.
Many factors, such as dietary intake, supplement use, cigarette smoking, alcohol drinking, and body mass index (BMI), are known to affect folate nutritional status [13-18]. However, there has been limited data of folate intake and blood levels and their association with health-related behaviors in Koreans. Therefore, our study aimed to assess folate intake from food and supplements and folate concentrations in the serum and RBCs, and investigate their association with some health-related behaviors in a sample of college students in Korea.
Subjects and Methods
Subjects
The study population consisted of healthy college students, 79 males and 90 females. They were recruited for the study through an advertisement on the Internet Homepage of Chungbuk National University located in Cheongju, Korea in March, 2009. After the nature and purpose of the study were explained, informed consent was obtained. This study was approved by the Institutional Review Board of Chungbuk Naitonal University Hospital (CBNU-IRB-BQ02).
Data collection of health-related behaviors
Information on the general characteristics and health-related behaviors, such as dietary supplement use, smoking, alcohol drinking, and physical activity, were gathered by a self-administered questionnaire. Height and weight were measured using an automatic height and weight measuring instrument (GL-150P, G-Tech, Korea).
Dietary assessment
Dietary intake data were collected by trained interviewers using a 24-hour recall method for three non-consecutive days in April, 2009. Energy and nutrient intakes were calculated by nutrient analysis software, DS24WIN program (Seoul National University, Korea). Folate values in this program were updated by substituting the new database published in the Korean Nutrition Society [19]. Folate intake from dietary supplements was calculated from the data on the name, amount and frequency of consumption of the supplements currently used regularly. Since the bioavailability of folic acid, a synthetic form used in dietary supplements is considered to be higher than naturally occurring food folates, a mixture of reduced folate polyglutamates, folic acid content in supplements is converted to an equivalent amount of food folate using the following equation, and total folate intake was expressed as 'dietary folate equivalents (DFE)'.
Blood sample collection and analyses
Blood samples were collected after an overnight fast, following a 3-day dietary survey. Blood samples were transported to the laboratory within two hours of collection and immediately processed. Whole blood, not containing anticoagulant, was separated by centrifugation to obtain the serum for folate analysis, and stored at -70℃. Blood samples to determine RBC folate and hematocrit were collected in EDTA-containing tubes. Hematocrit was measured by a hematology analyzer (Beckman Coulter AcT 10 hematology analyzer, USA) and whole blood was hemolyzed in potassium phosphate buffer (pH 4.5) containing 1% ascorbic acid. Folate concentrations were determined by microbiological assay using L. casei [20]. The coefficient of variation of the folate microbiological assay was less than 10%. All assays were performed within 3 months of sample collection.
Statistical analysis
Categorical variables were presented as frequencies and percentages, and χ2-tests were used to assess the differences between the groups. Numerical variables were given as the means and standard deviations (SD), and the differences of the means between the two groups were tested by a Student t-test. In order to examine the association between folate nutritional status and health-related behaviors, the variables for folic acid supplement use, smoking status, alcohol drinking frequency, amount of alcohol consumed at a time, physical activity, and BMI were categorized into the two groups. Total folate intake and blood folate concentrations of the corresponding categories were compared using a t-test for independent samples and a general linear model (GLM) for adjustment for potential confounding factors. Statistical significance was set at P < 0.05. All analyses were performed with the SAS software (Version 9.2, SAS Institute Inc., Cary, NC, USA).
Results
Characteristics of study subjects
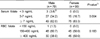
Table 1 shows age and anthropometric data of the subjects. The mean ages of male and female students were 22.7 and 20.9 years, respectively, ranging from 18 to 27 years. There were no significant differences in height, weight and body mass index (BMI) between males and females.
The characteristics of the study participants are shown in Table 2. While 26.6% of the students lived with parents, 72.4% of students lived independently. While 79.3% of the students were non-smokers, about 10% were either current or previous smokers. Approximately 11% of the students, especially 20% of males, had consumed alcohol at least three times a week. Students who engaged in physical activity for 30 min/day at least 3 times/week were 24.2%, and 36.1% of the students did not engage in any regular physical activity. There were significant differences in the type of residence, smoking status, frequencies of alcohol drinking and physical activity between male and female students. Approximately half of the students consumed dietary supplements, and only 14.8% took supplements containing folic acid.
Folate nutritional status
The mean dietary intakes and blood concentrations of folate are given in Table 3. Dietary folate intake was 429.4 µg and 328.7 µg in males and females, respectively. Total folate intake from diet and supplements in male and female students was 456.2 and 347.0 µgDFE, respectively, and these amounts were 114% and 87% of Recommended Nutrient Intake (RNI, 400 µgDFE), respectively. There was no significant difference when folate intake was expressed by energy intake between males and females.
The mean serum folate concentrations were 8.9 and 12.5 ng/mL, and the mean RBC folate concentrations were 398.6 and 405.3 ng/mL, respectively, in male and female students. Both the serum and RBC folate concentrations were lower in males than in females, even though total folate intakes were higher in males than females. The sex difference was only significant for the serum folate concentration. The proportions of male and female students who consumed less than Estimated Average Requirement (EAR, 320 µgDFE) were 21.5% and 45.6%, and those who consumed more than RNI were only 58.2% and 28.9%, respectively (Fig. 1).
The percentages of female students with serum folate value ≥ 7 ng/mL and RBC folate value ≥ 400 ng/mL, known as concentrations associated with the lowest risk of having an NTD-affected pregnancy were 83.3% and 50.0%, respectively (Table 4). None of the female students had serum and RBC concentrations below the cutoff for biochemical deficiency of 3 ng/mL and 150 ng/mL, respectively. However, 3.8% and 1.3% of the male students had deficient folate concentrations.
Association between folate nutritional status and health-related behaviors
Table 5 shows folate intake and its association with health-related behaviors. Total folate intake in male students was significantly higher in folic acid supplement users and those who practiced physical activity for 30 min/day at least three times per week. When folate intake was adjusted for energy intake, supplement use, non-smoking, less frequent alcohol drinking (< 1/wk) and regular physical activity were found to be associated with higher folate intake. Total folate intake in female students was significantly higher in folic acid supplement users, nonsmokers (including ex-smokers) and those who consumed < 2 drinks of any kind of alcoholic beverages at a time. Total folate intake after controlling for energy intake was higher in supplement users, those who consumed < 2 drinks of alcoholic beverages at a time, and exercised regularly for 30 min/day (≥ 3/wk) in females.
The serum folate concentrations according to health-related behaviors were shown in Table 6. Significantly higher serum folate concentrations were found in male students who consumed total folate ≥ EAR and used folic acid supplements. Smokers showed significantly lower serum folate concentrations than non-smokers both in males and females. The mean serum folate concentrations of ex-smokers were between the mean values of current smokers and non-smokers. Since only two female students were current smokers and two were ex-smokers, those two groups were combined as smokers, while ex-smokers were classified as non-smokers in male students. Frequent drinkers (≥ 1/wk) had lower serum folate concentrations than less frequent drinkers (< 1/wk) in males, and those who always consumed ≥ 2 drinks of any kind of alcoholic beverages at a time had significantly lower serum folate compared to those who consumed < 2 drinks at a time and non-drinkers in females. Regular physical activity for 30 min/day (≥ 3/wk) was found to be associated with significantly higher serum folate in males, and BMI ≥ 25 was associated with significantly lower serum folate in females. When serum folate concentration was adjusted for total folate intake, folic acid supplement, and health-related variables within the table, serum folate was associated with supplement use and physical activity in males and alcohol amount in females.
Table 7 shows RBC folate concentrations according to health-related behaviors. Significantly higher RBC folate concentrations were associated with supplement use, less frequent drinking, and regular physical activity in males, and less amount of alcohol at a time and regular physical activity in females. When RBC folate concentration was adjusted for total folate intake, folic acid supplement, and other health-related variables within the table, RBC folate was significantly higher in supplement users and those who practiced regular physical activity in males, and physically active females.
Discussion
We assessed folate intake and blood concentrations, and investigated the association between folate status and health-related behaviors among healthy Korean college students. Although the average total folate intakes were above RNI in males and 87% of the RNI in females, 21.5% of males and 45.6% of females did not meet the EAR (320 µgDFE). However, no female students were classified as folate deficient on the basis of 3 ng/mL of serum and 150 ng/mL of RBC concentrations. Furthermore, 50.0% of female students reached 7 ng/mL of serum and 400 ng/mL of RBC concentrations, which are considered as NTD-protective levels.
The mean concentration of serum folate was significantly lower in men compared to women, which is consistent with the previous studies [12,21-24]. In addition, the percentages classified as folate deficient on the basis of a 3 ng/mL cutoff point were higher in men compared to women. Male students had higher mean folate intakes, but there was no difference when expressed by energy intake between males and females. Further studies are needed to elucidate gender difference of the serum folate concentrations.
Comparison of dietary folate intake between countries may be difficult because of the differences in data collection method and food folate databases, as well as the differences in the inclusion of fortified food products and supplements for estimation of folate intake [25]. The average folate intake widely ranged from 200 to 450 µg/day in adults in Europe where folic acid fortification policy is not mandatory [26,27]. Our folate database is recently updated with the values analyzed microbiologically after trienzyme extraction [24], and we included folic acid intake from dietary supplements even though only 14.8% of students used folic acid supplements.
Low prevalence of serum folate deficiency could be explained by high consumption of Kimchi and rice. Kimchi and rice are the main sources of folate in Koreans, which contributed about 30~40% of folate intake [24]. Mito et al. [28] reported that the mean serum and RBC folate concentrations in Japanese pregnant women who were not consuming folic acid supplements were 10.3 and 519 ng/mL, respectively, which were higher than reported in other countries.
When folate intake was adjusted for energy intake, supplement use, alcohol drinking, and regular physical activity were found to be associated with higher folate intake in both male and female students.
Lower serum folate concentrations have been reported in smokers than in nonsmokers [14,17,18,29]. Our results also showed that serum folate concentrations were significantly lower among smokers, both in males and females. However, after controlling for other health-related variables including folate intake, no significant association was found between smoking and serum folate concentrations. In addition, there was no significant difference in RBC folate between smokers and non-smokers, which was different from the previous studies [14,29]. This may be due to the younger age and shorter period of smoking in our study subjects.
There is some evidence supporting an association between excessive alcohol consumption and inadequate folate status [13]. Alcohol may impair intestinal absorption and increase the urinary excretion in addition to lower diet quality. We also found that frequent drinkers (≥ 1/week) in men had significantly lower serum and RBC folate concentrations. However, after controlling for other health-related variables, no significant association was found between alcohol drinking frequency and serum or RBC folate concentrations. In female students, folate intake and serum/RBC folate concentrations were affected by the amount of alcohol consumed at a time rather than the frequency. Women who always consumed more than two alcoholic drinks at a time had significantly lower folate intake and serum and RBC folate concentrations. In addition, even after controlling for other health-related behaviors, there was a significant association between folate intake and serum concentrations with the amount of alcohol in female students. In a large prospective cohort study of more than 80,000 women [30], the investigators observed that very low dietary folate intake was more common among women who drank regularly, and the positive association between heavy alcohol/low folate intake and risk of major chronic disease was most apparent among women younger than 60 years of age. They concluded that adequate folate intake may be important in the primary prevention of the overall major chronic disease in women, especially among younger women consuming more than two alcoholic drinks per day. In some studies, moderate consumption of alcohol did not lower blood folate concentrations, and only excessive consumption seemed to lower folate concentrations, but it is surprising that a significant association was found between alcohol drinking and folate concentrations in this study participants who were female college students.
Higher BMI has been shown to be associated with lower serum folate concentrations in male and female adults [31], as well as in child-bearing age women [15]. Serum folate concentration in female students whose BMI is higher than 25 was significantly lower compared to those less than 25, but no association was found after controlling for other health-related behaviors. Since only 4 students was classified as BMI ≥ 25 and had low serum folate concentrations, further studies are needed to confirm the association of BMI and serum folate concentrations. There were no significant associations between BMI and RBC folate concentrations in both male and female students and these results are consistent with previous studies [15,31]. Our data shows that the students who practiced physical activity for 30 min/day three times or more per week had higher folate intake and blood folate concentrations even after controlling for other health-related behaviors. Others also reported that high serum folate and RBC folate concentrations were associated with high physical activity [17,32].
Our results indicate that the practice of desirable health-related behaviors, such as non-smoking, moderate alcohol drinking (< 1/wk, < 2 drinks at a time), regular physical activity (≥ 3 times/wk), and maintenance of healthy BMI, should be encouraged along with consumption of folate-rich foods and supplements in order to improve folate nutritional status among college students.







 XML Download
XML Download