

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Atopic dermatitis (AD) is a chronic inflammatory disease of the skin most commonly diagnosed in children; however, it can occur at any age. The prevalence of AD has been increasing in Korea, at a rate of 19.7% in 1995 to 27.5% in 2000; in 2003 and 2006, the rate soared to 33.1% among elementary school children and 34.9% among preschoolers, respectively [1-3]. These rapid increases are most likely due to environmental changes, although there is a clear genetic component in AD. It has been reported that a reduced barrier function as well as an altered immune function are fundamental causes of the development of AD [4].
Food allergies (FA) arise from a specific reproducible immune response that occurs with exposure to a given food [4]. The clinical spectrum of FA ranges from mild skin irritation to severe, life-threatening anaphylaxis. Currently, avoidance of the causative agent remains as the mainstay of FA management [4,5]. Food allergic or immunologic reactions are classified into three groups, including IgE-mediated food allergies (IFAs), non-IgE-mediated food allergies (NFAs), and mixed food allergies (NFA + IFA) [6]. NFAs were slower than IFAs in onset time and primarily resulted in gastrointestinal reactions. IFAs demonstrated rapid onset, with most cases resulting in anaphylaxis or urticaria. Table 1 shows the classification of NFA and IFA patients based on skin manifestations and time of onset.
The majority of FAs are mediated by IgE yet, sensitization to a specific food, as confirmed by the skin prick test (SPT) or serum-specific IgE, does not always imply clinical reactivity. Accurate diagnosis of FAs should be based on an open food challenge (OFC) [7]. Because there are no specific laboratory tests for NFAs, diagnoses are made using elimination diets and oral challenges [8,9], as well food challenge tests for confirmation of the FA [10,11]. Several food challenge methods have been proposed, including double-blind, placebo-controlled food challenges (DBPCFC) and OFCs [12]. In an OFC, the patient is not blinded and thus recognizes the test food. The test results are then interpreted according to the objective symptoms. If the patient displays anxiety about the challenge and complains of abdominal pain or pruritus, the food challenge test is considered invalid [13]. DBPCFC is considered to be a more accurate method for diagnosing FAs, as both the patient and the observer are blinded to the test food. This is the most rigorous method for diagnosing adverse food reactions [14]; however, it is difficult to perform DBPCFCs in a clinical setting.
In Japan, 70% of all patients who required treatment for acute allergic reactions had food allergies to eggs, milk, or wheat [15]. Ellman et al. [16] reported in the U.S., allergies to eggs, milk, wheat, soy, peanuts, tree nuts, and seafood account for up to 90% of food allergies in children with AD. In Korea, the prevalence of food allergies by OFC testing among patients with AD was as follows: milk; 67.3%, chicken; 64.2%, pork; 62.8%, eggs; 61.0%, beef; 55.4%, wheat; 52.0% and soybeans; 45.2%. Little research has been conducted on these 7 specific foods that have been shown to be the primary food allergens in Korea [17]. The aim of the present study was to investigate the characteristics of FAs in patients with AD. We determined the prevalence of types of food allergies, the prevalence of combinations of food allergies, the SCORing Atopic Dermatitis (SCORAD) index, and the onset time of allergic reaction in patients with AD.
Subjects and Methods
Subjects
A total of 2,417 patients (M:F = 1,222:1,195) who visited either the Department of Allergy and Clinical Immunology at the Seoul Allergy Clinic, Seoul, Korea or the Chungnam National University Hospital Pediatric Allergic Clinic, Daejeon, Korea between June 2000 and August 2010 were enrolled in this study (Table 2). The age groups were classified with respect to the physiological characteristics and developmental stages of infants, toddlers, children, adolescents, adults, and the elderly, as referenced by the age classification of the Korean Nutrition Society [18]. All subjects suffered from repeated eczematous reactions or exacerbations of AD. The subjects received blood tests and skin prick tests (SPTs), as described below, and fulfilled the criteria of Hanifin and Rajka [19]. Informed consent was obtained from adult patients or the parents of children participating in the study. This study was approved by the Institutional Review Board of Chungnam University, Daejeon, Korea.
Diagnosis of food allergy
Blood test
All subjects underwent blood tests and SPTs. Blood tests included a complete blood cell count (CBC) with differential in order to determine the eosinophilic fraction, total serum IgE levels, and food specific serum IgE levels (which were measured using UniCAP; Pharmacia & Upjohn Diagnostics AB, Uppsala, Sweden). Serum food-specific IgE levels less than 0.35 kU/L were classified as undetectable.
Skin prick tests
SPTs were simultaneously conducted on patients' left forearm using crude and commercial allergy extracts (Bencard, Brentford, England). Histamine hydrochloride (1 mg/ml, Bencard) was used as a positive control. SPTs using vehicles (physiologic saline, distilled water, and glycerol) were the negative controls. Reactions were read 15 min after the skin prick test and were classified as either negative (0; no reaction, +; reaction greater than the control reaction but smaller than half the size of histamine) or positive (++; half, +++; same, and ++++; twice the size of histamine). The minimum size for a positive reaction was 3 mm (+++).
Food allergens (1:10 or 1:20 glycerinated food extract) that elicited a wheal at least 3 mm larger than the negative control (not including erythema) were considered to be positive, while anything less than 3 mm was considered to be negative.
Food challenge test
Diagnoses of allergies to milk, eggs, wheat, soybeans, beef, pork, and chicken were made for all subjects via food challenge tests. Among the seven foods, milk, eggs, wheat, and soybeans were tested using DBPCFCs, whereas beef, pork and chicken were tested via OFCs. Food allergies were classified as IFA, NFA, and mixed types, based on the objective symptoms, as described in Table 1.
1) Elimination diet
A trial of an elimination diet preceded the food challenge test for all 7 foods. Patients were asked to eliminate the suspected allergen according to their past history of allergic responses, skin prick tests, and specific IgE (maximum elimination phase). A replacement diet was designed in order to provide substitutes for the eliminated foods in order to maintain a balanced nutrition [17]. To confirm the complete elimination of all foods identified as allergens, all patients were required to keep dietary diaries. The analysis of dietary diaries was performed by dietitians as well as physicians. In addition, the elimination diet was implemented to the mother's diet for breast fed infants.
2) Open food challenge tests
OFCs were performed according to the following indications (challenge phase): a) obvious clinical improvement was obtained and the clinical status was stable for at least 2 weeks, and b) the allergens tested were completely eliminated from the diet. This was confirmed via the analysis of the dietary diary by a dietician. To exclude possible environmental factors, patients maintained their daily living patterns as regularly as possible during the testing period.
Patients consumed one portion of the test food each morning [18]. Three days after the first challenge, the clinical results and the severity score were evaluated. If patients showed increased severity scores or obvious worsening of clinical signs or symptoms, the tests were discontinued. Otherwise, the food challenge tests continued with ingestion of increased quantities of the test food for another 4 days. If patients showed worsening symptoms, the subsequent challenges were delayed until patients recovered to the pre-challenge state. If patients consumed the food that was to be eliminated during the study, the challenge tests were ceased and the patients were observed for 1 week.
3) Double-blind placebo-controlled food challenges
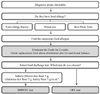
The recipes for DBPCFCs using eggs, milk, and soybeans were developed by dieticians at the Seoul Allergy Clinic. The vehicle used was 15 g of mixed cereal flour, consisting of brown rice flour (5 g), glutinous rice flour (5 g), and barley flour (5 g). For the DBPCFC, a 21 g mixture, consisting of 15 g of the above mixed cereal flour and 6 g of freeze-dried eggs, soybeans, or skim milk powder, was used. Foods that contained eggs, milk, and soybeans were eliminated from daily diets for at least two weeks prior to testing. Before starting the DBPCFC, it was confirmed that the patients tolerated mixed cereal flour by challenging them with the placebo for 7 days. If no symptoms were reported, patients proceeded with the DBPCFC. Two challenges, separated by a period of 7 days, were performed including one with placebo only and one with the suspected food antigen within the vehicle. Fig. 1 summarizes the diagnostic flow of the food challenge tests in patients with atopic dermatitis.
Clinical severity scoring of food allergy
The clinical severity of NFA was assessed using the SCORAD index, a system used worldwide to assess the severity of atopic eczema [20]. A diagnosis of FA was made if the clinical severity score increased by > 20% in subjects demonstrating a baseline score > 50 points, or if the score increased by > 10 points for those with a baseline score ≤ 50 points. New skin lesions and itching were regarded as positive reactions, which were required for the diagnosis of FA by the food challenge test. The clinical severity of IFA was estimated using a slightly modified Clark's scoring system [21]. Positive reactions were assigned 5 points, onset times < 15 min were assigned 10 points, and onset times > 15 min were assigned five points. Clinical severity scores for IFA ranged from 10 to 30 points.
Results
Food allergy prevalence
The prevalence of food allergies was 50.7% (1,225/2,417) in patients with AD (Table 2). Patients aged 0-11 months and over the age of 30 showed a FA prevalence of less than 50%. However, patients aged 1-29 years showed a FA prevalence from 53.8%-61.1%, which is higher than other age groups. The type of FA was classified as NFA, IFA, or mixed. The prevalence of NFA was 94.9% (1,162/1,225), IFA was 2.2% (27/1,225), and mixed was 2.9% (36/1,225). Subjects aged 65 and older were presented with only NFA, However, all other age groups showed a combination of NFA, IFA, and mixed (Table 2).
The prevalence of FAs to the 7 food items tested in patients with AD were eggs; 21.6% (523/2,417), milk; 20.9% (506/2,417), wheat; 11.8% (285/2,417), soybeans; 11.7% (282/2,417), chicken; 11.7% (283/2,417), pork; 8.9% (216/2,417), and beef; 9.2% (222/2,417) (Table 3). The most prominent type of FA was NFA, however, milk and eggs more commonly caused IFA when compared to other foods. Beef did not cause IFA.
Among patients with FAs, the prevalence of allergies to the various numbers of food items is shown in Table 4. The prevalence of reactions to 1 food was 45.1% (553/1,225); to 2 foods, 30.6% (375/1,225); to 3 foods, 15.3% (187/1,225); to 4, foods was 5.8% (71/1,225) to 5 foods, 2.2% (27/1,225); and to 6 foods, 1.0% (12/1,225).
We examined the characteristics of 2 FA combinations (Table 5), and found that 28.5% (149/523) of FA patients allergic to eggs were also allergic to milk. Likewise, 29.4% (149/506) of FA patients allergic to milk also were allergic to eggs. Patients with an allergy to one of the other 5 foods tested had a concomitant allergy for eggs or milk more frequently than other foods. For example, 43.5% (124/285) of FA patients with wheat allergy, 42.0% (119/283) with chicken allergy, 41.7% (90/216) with pork allergy, 39.2% (87/222) with beef allergy, and 38.3% (108/282) with soybean allergy also had egg allergy.
Table 6 presents the prevalence of allergies to all 7 food items according to age. In all ages, the prevalence rates of allergy to eggs and milk were higher than that of any other foods. In particular, FA prevalence of milk in patients aged 0-5 months and 6-11 months showed a rate between 14.8-24.7%, which is the lowest rate among all age groups, whereas patients over the age of 1 year showed a FA prevalence of 37.5-55.1%. FA prevalence of soybean in patients aged 6-11 months showed 34.8% which is the highest rate among all age groups.
Characteristics of clinical severity in the food challenge test
Severity
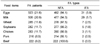
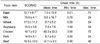
Table 7 shows the score differences for clinical severity during the food challenge test. The score differences were obtained by subtracting the scores of the pre-challenge test from those of the post-challenge test. The results ranked from greatest to least: wheat, beef, soybeans, milk, pork, eggs, and chicken.
Onset time, maximum time, and minimum time to food allergy reaction
With regards to the mean onset time of the FA reaction, the shortest time to reaction was seen in wheat (6.7 ± 8.2 h), and the longest was seen in chicken (45.3 ± 22.2 h). The minimum and maximum onset time of FA reactions were different between food items: wheat (min = 0.20 h; max = 24 h), beef (0.50 h; 48 h), soybeans (1.0 h; 24 h), milk (0.70 h; 24 h), pork (3.0 h; 24 h), eggs (0.01 h; 72 h),and chicken (3.0 h; 72 h) (Table 7).
Discussion
Over the last several decades, studies involving controlled food challenges have provided a reliable scientific understanding of the role of foods in hypersensitivity reactions. Most of these investigations have focused on pediatric populations, and as a result, less evidence for adverse reactions to foods in adults has been reported. In our study, the prevalence of FAs was 50.7% (1,225/2,417) in patients with AD. We also examined changes in the prevalence of FAs by age. Less than 40% of patients aged 0-11months and over the age of 30 demonstrated FAs. This is consistent with previous reports that the prevalence of FA in infants with atopic dermatitis ranges from 30-40% [15,16,22]. Patients aged 1-29 years, however, showed a FA prevalence of more than 50%. These results are consistent with another study [23] in which the prevalence of FAs increased with age (1-18 years) in Australia, China, Taiwan, Japan, and Malaysia. Overall, food allergies tended to begin at an early age and were more frequent in children than in the adult population. Our data suggest that the prevalence of FAs gradually increases between the age of 1-2 and declines after the age of 19-29.
The types of FAs were classified as NFA, IFA, or mixed. Among patients with AD, the major type of FA was NFA (94.9%, 1162/1,225), whereas IFA (2.2%, 27/1,225) and mixed (2.9%, 36/1,225) were significantly less common. Subjects older than 65 years of age were only presented with NFA; however, all other age groups showed a combination of NFA, IFA, and mixed. Eigenmann et al. [24] reported that about 35% of children with AD have IFA, as determined by DBPCFC. Additionally, some studies [25,26] have shown the FA prevalence in infants with AD to be 30%. The most common allergy, among the seven foods (milk, eggs, wheat, soybean, beef, pork, and chicken), tested in our study was eggs (21.6%), followed closely by milk (20.9%). The FA that was least frequently observed was pork (8.9%). A previous study demonstrated positive FA rates of 36.7% to egg whites, 34.8% to wheat, 31.7% to milk, and 30.4% to soybeans [27]. As determined by DBPCFC, the prevalence of specific FAs varies according to different reports. For example, the prevalence of milk allergies in patients with AD was reported to be 33.3% or 50% in two separate studies [28,29]. Likewise, the prevalence of soybean allergies was 11.7% in our study; however, this varied widely from 33.3% [28], to 28% [29], and to 3.1% [30] in other studies. Milk and eggs have been reported to be the most frequent causes for food allergies in AD, with the highest rates belonging to egg allergies [25,31-35]. NFA was overall the most common type of FA observed in our study; however, eggs and milk showed higher IFA responses compared to other foods. Interestingly, only beef did not show an IFA response, and the prevalence of FA to meat (beef, pork, and chicken) was lower than that of other foods (milk, eggs, wheat, and soybeans). Eggs and milk are often components of creamy salad dressings, pastas, whipped cream, icing, batters, and many other food preparations. As a result, many patients with these food allergies are often unable to eat baked goods. These are important allergies to be aware of, as reactions may occur immediately and range from mild to life threatening, in cases of anaphylaxis. In this study, the prevalence of milk allergy sharply increased from 1-2 years. The increase is attributed to whole milk consumption, which begins after breastfeeding or the consumption of modified milk formula. Cow's milk is usually the first food given to an infant, and cow's milk hypersensitivity is often the first symptom of an atopic condition. Cow's milk allergy often disappears before the age of 1 year. Associated reactions to other foods develop in approximately 45% of patients [36].
Among FA patients, the prevalence of 1 FA was 45.1% and 2 FAs was 30.6%. Additionally, the prevalence of more than 3 FAs was 15.3%. The food combination which showed the highest prevalence of two FAs was egg and milk in both NFA and IFA type reactions. Thus, patients with FAs have a high probability of having egg and milk allergies.
The food which showed the most severe reaction and the earliest onset time was wheat. Chicken, on the other hand, had the least severe reaction and the latest onset time. In many previous studies, most of the reactions occurring during the OFC were immediate, while delayed reactions were more controversial [37,38]. In other studies, skin manifestations continued to appear up to 7 days after exposure [38,39].
Our results suggest that the management of FAs is vital for improving symptoms of AD. Over the course of the food challenge, nutritional management was required, and dietary guidelines were collectively developed by the patient, dietitian, and physician. Reactions to food items also had variable onset times and levels of severity. As our study examined only 7 common foods, further research will be necessary for the development of a more comprehensive dietary guideline.





 XML Download
XML Download