

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Atopic dermatitis (AD) is a chronic pruritic skin disease and usually starts during early infancy. AD in infancy and early childhood could also be considered as a preceding stage towards the progression to other atopic diseases such as asthma, allergic rhinitis, and severe allergic reactions to foods over time, which is called the atopic march [1]. The study comparing the International Study of Asthma and Allergies in Childhood (ISAAC) for phase one (1992-1998) with phase three (1999-2004), repeating multi-country cross-sectional surveys, reported that the worldwide prevalence of allergic diseases has been increasing [2]. Numerous investigations showed that the prevalence of AD in young children has consistently been increasing in most Western countries as well as some Asian counties such as South Korea, Taiwan and Japan; overall, up to 20% of children have suffered from AD [2-4].
Although the cause of AD is not fully understood, previous studies proposed that AD is probably affected by multiple issues including genetics, environment, and dietary factors [5,6]. In respect of the etiology of AD, a proposed mechanism relating to genetic and environmental factors is the epidermal barrier defect induced by reducing lipids such as ceramide and spingosine or dysfunctional filaggrin, an epidermal barrier structural protein [7,8]. This skin barrier dysfunction could activate immune responses and promote inflammatory responses through the increased penetration of allergens [7,8].
However, dietary factors could be more important than genetic and environment factors to investigate AD in the young children group because AD has shown distinctive features depending on age. Infancy and young children have been known to be more allergic to food, while environmental antigens were common in adults [9,10]. Previous studies reported that food allergies have been accompanied in approximately 35-40% of children with AD [5,11,12]. Based on the association between food allergies and AD, a variety of treatments reducing food allergies or preventing AD have been suggested, which were maternal dietary restrictions during pregnancy and lactation, exclusive breastfeeding, usage of a hydrolyzed formula, delayed introduction of solid foods, and other nutritional interventions [13-15]. Antioxidant nutrients have also been suggested as one of the possible treatments to decrease allergic and inflammatory responses by the reduction of oxidative stress. Indeed, increased oxidative stress and impaired homeostasis of oxygen/nitrogen radicals were observed in children with AD [16]. Consequently, antioxidant vitamins and polyunsaturated fatty acid (PUFA) like n-3 and n-6 fatty acids relating to AD have received notable attention [17-21].
In patients with AD, elevated total IgE or specific IgE antibody levels were commonly observed [9,22]. Thus, to diagnose AD and its severity, determining total IgE levels and specific IgE levels to common allergens in the blood was proposed as a useful tool in the pediatric population [23,24].
Many epidemiologic as well as clinical interventional studies to research the effect of dietary antioxidant vitamins and PUFA have reported to decrease serum IgE levels and to decrease the development or severity of AD; however, their outcomes have been inconsistent [13,18,25,26]. Besides, vitamin E supplementation decreased 62% of serum IgE levels based on the initial serum IgE level [27]. Also, a clinical trial on 52 AD patients, aged 13-45 years old reported a significant negative association between plasma vitamin E and SCORing Atopic Dermatitis (SCORAD), which is used for the diagnosis of AD and its severity [28].
Therefore, we aimed to investigate the association between dietary nutrients including PUFA and, vitamin C and E which are the most potent antioxidants and scavenger of oxidative radicals, and serum total IgE/specific IgE levels in infants and young children with AD.
Subjects and Methods
Subjects
This is a cross-sectional study. A total of 119 (male 79 and female 40) infants and young children with atopic dermatitis were recruited from those who had visited the allergy center at Samsung Medical Center, Seoul, Korea from March 2008 to September 2009. We only included infants and young children aged 0-24 months diagnosed with AD by a pediatrician according to diagnostic criteria by Hanifin and Rajka [29]. Informed consents were obtained from the parents of all participants and the study protocol was approved by the Samsung Medical Center Ethics Committee.
Laboratory analyses
The serum levels of total IgE (n = 113) and allergen-specific IgEs to the six predominant food allergens; egg whites (n = 112), milk (n = 110), wheat (n = 111), buckwheat (n = 102), soy (n = 110), and peanuts (n = 107) were measured by CAP-FEIA (Immuno CAP 100E, Pharmacia, Uppsala, Sewden). Serum vitamin E (α-tocopherol) concentration in 25 of the total participants was estimated by HPLC at the Eone Reference Laboratory, Seoul, Korea.
Dietary intake assessment
A previous day's 24-h diet recall was used to assess the dietary intake of infants and young children. The 24h recall data were collected face to face by trained interviewers from their mothers and analysed through the use of a Computer Aided Nutritional Analysis Program (CAN-pro version 3.0) developed by the Korean Nutrition Society.
To estimate breast milk intake we adapted the assumptions of the feeding infants and toddlers study (FITS) [30,31]. However, we also adjusted the total quantity of breast milk from 780 ml/day to 750 ml/day for infants' aged 0-5 mo based on the previous studies which were performed in Korean infants and young children. Thus, for infants aged less than 5 mo who had breast milk only as milk, the total breast milk intake was assumed as 750 ml per day. For infants who consumed breast milk and formula together, the volume of formula was subtracted from 750 ml to calculate the quantity of breast milk consumed. For infants aged older than 5 mo, the quantity was 600 ml per day as the total breast milk intake in case of those who received only breast milk as milk. For infants who consumed breast milk with formula or other milk such as cow's and goat's milk simultaneously, the volume of formula or other milk was subtracted from 600 ml to estimate the quantity of breast milk consumed. We also asked all participants about supplement use.
Demographics
Demographic information on parents' age, age of onset, duration of AD, and family history (atopic dermatitis, asthma, allergic rhinitis etc.) was obtained.
Statistical analysis
Student's t-test was applied to compare the differences between males and females in general characteristics, dietary intakes, serum vitamin E and serum IgE levels. Multiple linear regression analysis was used to evaluate the relationships between serum IgE levels and the consumption of each nutrient, as well as between serum IgE and serum vitamin E levels. After adjusting for age, gender, and total energy intake, the β coefficients, 95% confidence intervals, and P-values were calculated by the general linear model (GLM). All statistical analyses were performed using the SAS package version 9.1 (SAS institute, Cary, NC, USA). A P-value of 0.05 was considered statistically significant.
Results
General characteristics and nutrient intakes of subjects
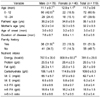
Participants included 119 infants and young children (male 79 and female 40) with AD who were 0-12 mo old (n = 72, 60.5%) or 13-24 mo old (n = 47, 39.5%) (Table 1). The mean of onset age of AD was 3 mo-old and they had suffered from it for 8 mo on average. Roughly, half of the participants (51.3%) reported a family history relating to allergic diseases such as AD, asthma and allergic rhinitis. Fathers of 36% and mothers of 21% in regards to infants and young children reported history of allergic diseases. In Table 1, mean dietary intakes were shown. The average for energy intake was 781.6 kcal/d. The dietary intake of vitamin C and E was higher than the values of the dietary reference intakes for Koreans (DRIs) in all participants (vitamin C; recommended nutrition intake (RNI) for a young child aged 1-2 yr, 40 mg/day, and vitamin E; adequate intake (AI) for one aged 1-2 yr, 5mg α-tocopherol/day). No significant differences were observed between males and females in nutrient intake. We also included questions about the use of supplements. All participants did not take any supplement at the time of study. Mothers of three participants responded that their children had used supplements such as Chinese medicine, omega-3 fatty acid, lactobacillus and antioxidant vitamin products. Thus, the effect of supplement use seemed to be negligible on the association between dietary intake and serum IgEs.
Serum IgE and vitamin E levels
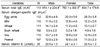
We measured serum levels of total IgE and allergen-specific IgEs to the six predominant food allergens which were egg whites, milk, wheat, buckwheat, soy, and peanuts to determine food hypersensitivity. Total serum IgE levels < 300 kU/l were considered in the normal or borderline range [32] and specific IgE levels ≥ 0.35 kUA/l (RAST class ≥ 1) by CAP assay were considered positive [33]. Children in the study showed high total serum IgE and specific IgE levels regardless of gender (Table 2). In general, the higher those levels rise, the more severe AD is considered. The mean of serum vitamin E levels was 22.5 µmol/L. There was no difference between males and females in both serum IgEs and serum vitamin E levels. Serum vitamin E demonstrated a significant inverse association with serum total IgEs as well as specific IgEs to the six food allergens (P < 0.05, Table 3). The statistical significance was not changed by adjustment for age and gender.
The relationship between serum IgE levels and nutrient intakes
In Table 4, the serum total IgE level was positively associated with CHO (P < 0.05). Positive associations were also found between CHO intake and specific IgEs to egg whites, milk, soy, and peanuts (P < 0.05). Negative associations were found between protein intake and specific IgE to egg whites. Fat intake was also inversely related with specific-IgEs to egg whites, milk, buck wheat, soy, and peanuts (P < 0.05). Vitamin E intake was positively associated with buck wheat, but no others (P < 0.05). In addition, serum vitamin E showed no relationship with dietary vitamin E by Pearson's correlation analysis regardless of adjusting age and gender (data not shown). There were no associations between vitamin C and n-3/n-6 fatty acids, and serum IgE levels.
Discussion
To study the association between antioxidants; vitamin C and E, and PUFA and serum IgE levels served as a predictor and diagnostic criteria of AD in infants and young children. Also, we only included those aged 0-24months who were diagnosed with AD by a pediatrician who also measured dietary intake as well as blood indices (total IgE, allergen-specific IgEs, and serum vit E). Serum vitamin E concentration might be a good indicator of dietary vitamin E intake [34]; unfortunately, we were only able to measure serum vitamin E levels in 25 children out of the total 119 participants because they were aged less than 24 months and there was difficulty in terms of the limited amount of blood drawn. Nevertheless, we found that the serum vitamin E level drew a remarkable negative relationship with serum total IgE and specific IgE levels. To see whether 25 children used in the serum vitamin E analysis are a representative group, we compared serum IgEs and dietary intake between the 25 children and the rest of the children by student's t-test and found no significant differences. Therefore, we postulated that the result implicates the association of serum vitamin E and serum IgEs.
To our knowledge, there were limited studies to investigate directly the association between serum vitamin E and serum IgE levels. Some studies have reported similar outcomes in terms of the relation between serum vitamin E and IgEs, yet they used different endpoints. They reported that plasma vitamin E was significantly negatively associated with SCORAD, an indicator of AD's severity and the prevalence of eczema in Japanese children aged 10-13 yr old [28,35]. In adults with higher serum vitamin E level, less allergic skin sensitization was observed [36].
There are two primary possible mechanisms related to ameliorate AD. One may be vitamin E's function as a potent antioxidant vitamin. Vitamin E is very well known as a chain-breaking antioxidant that prevents the propagation of lipid peroxidation, which protects PUFA within the membrane from oxidative damage [37,38]. Omata et al. [16] reported that increased oxidative stress could be involved in the pathophysiology of childhood AD and suggested the suppression of oxidative stress as a useful strategy regarding the treatment of AD. Another possible mechanism may be the immune response effect of vitamin E. A critical review about vitamin E and the immune response in the aged reported that vitamin E can enhance the T-cell-mediated function by directly affecting T cells, and indirectly by reducing macrophages and prostaglandin E2 production [39]. In vivo and vitro studies supporting vitamin E may reduce prostaglandin E2, which is the monocyte-derived inflammatory mediator, thereby decreasing IgE synthesis by increasing IFN-γ production in AD [40,41]. It could be also provided as evidence for the fact that higher concentrations of vitamin E intake were associated with lower serum IgE concentrations and a lower frequency of allergen sensitization in humans [42].
We also expected that some nutrients have an inverse relation with serum IgE and specific IgE levels. However, we found no significant associations between nutrients (vit C and E, and PUFA) and total IgE and allergen-specific IgE, except the positive relation between vit E and specific IgE level to buckwheat (P < 0.05).
Consistent with our results, Petal et al. reported that vitamin E intake was positively associated with an allergic sensitization at the age of 5 amongst children, but not at the age of 8 [43]. Several studies also reported that vitamin E intake could be irrelevant to serum IgE levels or allergic diseases [20,43,44].
Conversely, in a vivo study examining the effect of antioxidants on the IgE production-regulating activity of unsaturated fatty acids (UFA), vitamin E showed to counteract the stimulated IgE production by arachidonic acid, but vitamin C was not effective [41]. Several human studies also reported that dietary vitamin E could decrease serum IgE levels. Oh et al. [45] also showed 1 standard deviation increase of serum vitamin E reduced AD risk in Korean children [OR = 0.64, 95% CI = 0.41-0.98]. In 2,498 adults, a significant inverse relationship between dietary vitamin E and serum total IgE levels was shown with adjustment for age, sex, and smoking. Moreover, daily dietary vitamin E intake was inversely and independently associated with a reduction in the risk of atopy [42]. In a single-blind clinical study, a vitamin E supplement in individuals with AD demonstrated a decrease of 62% in serum IgE levels based on the initial condition [27]. The outcomes of studies to investigate the relation between dietary vitamin E and serum IgE levels have been inconsistent; therefore the study results should be interpreted cautiously.
Likewise, the results of studies investigated the effect of other dietary factors; vitamin C and n-3 /n-6 fatty acids on AD were inconsistent [17-21]. Women with AD were observed to have lower dietary intake of foods rich in the antioxidant vitamin C, such as oranges and orange juice, but no correlation was found between these foods and AD clinical severity scores [46]. Also, a case-control study in Korean children with AD showed no association between dietary and plasma vitamin C and AD risk [45]. Some studies have shown that dietary vitamin C was unrelated to allergic diseases [43,44]. On the other hand, in relation to n-3/n-6 fatty acids, Finch et al. suggested that they may not be effective in preventing AD, but have some benefits on decreasing the severity of AD [13].
In addition, fat and protein intakes showed an inverse relationship with most serum specific IgEs. Although serum IgE levels were not measured, a study based on ISAAC data; a multi-country cross-sectional survey, similarly reported a negative association between atopic diseases and fat, protein and specific vegetable nutrients (vit A, vit E, MUFA, PUFA, and saturated fat) [18]. While dietary fat showed a significantly negative association with five food allergens specific IgEs to egg whites, milk, buck wheat, soy and peanuts, dietary carbohydrates (CHO) were strongly positively related with specific IgEs to egg whites, milk, soy, and peanuts (P < 0.05). This result was contraryto the one by Trak-Fellermeier et al. [47], which demonstrated a positive association between high fat intake and allergic sensitization. One possible explanation for the result could be that Korean mothers having children with AD have a trend to restrict dietary fat or food rich in fat as an aggravating dietary factor and to avoid western diets known for increasing the prevalence of AD (data not shown); thus, CHO intake might be relatively increased.
In general, milk, soy, eggs, wheat, and peanuts have been reported as the most common food allergen in children in both Western and Asian countries [9,12,48]. The predominant food allergens could appear differently according to age and culture. Thus, we included buckwheat to the list of predominant food allergens because buckwheat (except milk, soy, eggs, wheat and peanut) has been distinguishably reported as one of the dominant food allergens in some Asian countries such as Korea and Japan [9,49]. A study showing the rate of sensitization to food allergen in Korean children including those aged less than 3yr reported that buckwheat was highly ranked among food allergens [9]. A national survey in Japan also showed that buckwheat was among five major food allergens, along with eggs, milk, wheat, and peanuts [49].
Our study has some limitations. The inconsistency of the study results about dietary intake and AD could be caused by dietary intake assessment tools. Most studies generally used either validated semi-quantitative food frequency quantitative (FFQ) or multiple 24h-recalls to assess usual dietary intake. To the best of our knowledge, there are no validated FFQs to assess the dietary intake of infants and young children in Korea. Furthermore, we were only able to collect one-day 24h-recalls; therefore, it may not reflect the usual dietary intake of infants and children, which might be the primary reason that we were not able to prove an inverse association between dietary intake and serum IgE levels. Even though we had some limitations in the current study, serum vitamin E showed a strong negative association with serum IgE and specific IgE levels. The finding indirectly indicated that dietary vitamin E intake could play an important role in allergic responses or AD in children.
In conclusion, our findings in the study suggest that higher serum vitamin E levels possibly reduced serum IgEs, which may implicate that a high consumption of dietary vitamin E has a positive effect to ameliorate AD symptoms in infants and young children. For further study, it could be suggested to develop FFQ and validate FFQ for the investigation regarding the association between dietary intake and AD in infants and children.


 XML Download
XML Download