

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Statins are HMG coA reductase inhibitors and are one of the most popular cholesterol-lowering drugs in humans. Among US adults aged ≥ 40 years with hypertension, 14.5% are taking statin medications based on the NHANES (1999-2002) [1], and an increasing number of the Korean population is using statin therapy. Besides their cholesterol lowering effect, statins are effective for preventing cardiovascular diseases such as stroke, myocardial infarction, and hypertension [2,3].
The beneficial effects of statins include preservation of bone minerals [4] and prevention of beta amyloid accumulation [5] and cell apoptosis [6]. However, muscle dysfunction such as myalgia and cardiomyopathy have been reported as statin-associated adverse effects [7,8]. Statins deplete ubiquinone, which is involved in the cholesterol biosynthetic pathway. Endogenous ubiquinones such as coenzyme Q10 (CoQ10) are essential electron carriers in the mitochondrial electron transport system (ETS) of active muscle. Statin users with myopathic symptoms have lower CoQ10 muscular concentrations [9], and CoQ10 supplementation reverses the decreased plasma CoQ10 and alleviates myalgic symptoms following statin therapy [8]. Dhanasekaran and Ren [10] reviewed the beneficial effects of CoQ10 on preventing neurodegenerative disorders, cancer, cardiovascular diseases, diabetes mellitus, aging, and Alzheimer's disease.
CoQ10 in mammals has a hydrophilic benzoquinone ring with a lipophilic side chain of 10 isoprene units embedded in a hydrophobic membrane core. The benzoquinone head exists in three different redox states: the fully oxidized form ubiquinone, the partially reduced free radical form ubisemiquinone, and the fully reduced form ubiquinol [11]. Maroz et al. [12] suggested that ubiquinone scavenges superoxide in the ETS, whereas ubiquinol scavenges other oxygen radicals and carbon-centered radicals, indicating that ubiquinol may play a role preventing membrane lipid peroxidation. López-Lluch et al. [13] proposed that CoQ10 in the plasma membrane participates in regenerating alpha-tocopherol and ascorbate from their radical forms and prevents loss of antioxidant capacity and membrane damage.
Platelet activation and the platelet release reaction may be affected by conditions such as oxidative stress and platelet lipids. Plant polyphenols decrease the platelet response and release reaction, thereby suppressing platelet aggregation and superoxide production [14,15]. Reduced CoQ10 improves platelet mitochondrial function by protecting platelets from oxidative stress [16]. Statins affect platelet aggregation by modulating platelet cholesterol [17]. Atorvastatin decreases cholesterol content in erythrocyte membranes by decreasing the cholesterol/phospholipid ratio, which provides membrane stability and increased Na-K ATPase activity in guinea pigs [18]. Changes in membrane lipid composition and peroxidation may cause alterations in membrane cation channels that are associated with clinical complications such as hypertension, pregnancy, and diabetes. Increased erythrocyte Na-Li counter-transport activity is correlated with increased membrane cholesterol/phospholipid ratio in patients with essential hypertension [19]. Elevated erythrocyte Na-pump activity, Na-K co-transport and Na-Li counter-transport, and decreased erythrocyte membrane phospholipid content were are observed in patients with insulin dependent diabetes [20]. Abnormally low erythrocyte Na-K co-transport activity is associated with red blood cell (RBC) deformities and membrane permeability in patients with pregnancy-induced hypertension [21].
The evergreen shrub Ardisia japonica Blume (AJB) is native to eastern China, Japan, and Korea. It is considered one of the 50 fundamental herbs in traditional Chinese medicine, called zijinniu, and is used to treat cough, cancer, poisons, and tuberculosis and improves diuresis and blood circulation [22]. Kobayashi and de Mejia [23] reported that ardisin, ardisianone, berginin and embelin in A. japonica have anti-allergenic, antihuman immunodeficiency virus, anti-cancer, and hypoglycemic effects as well as strong antioxidant activity. Ardisianone and benzoquinone from A. japonica have an inhibitory effect on 5-lipoxygenase [23], and triterpenoid saponins from A. crenata stimulate cAMP phosphodiesterase activity [24]. Besides rich in triterpenoids of isoprene units, genus Ardisia contains 2-hydroxy-5-methoxy-3-pentadecenyl-benzoquinone, which is structurally similar to the benzoquinone nucleus of coenzyme Q (2,3 dimethoxy-5-methyl-6-dedecaprenyl-benzoquinone) [23,25].
Interests in complementary and alternative medicine have increased to prevent and therapeutically treat certain diseases using a "natural" and "safe" method despite a lack of scientific evidence for their efficacy. In this study, we investigated the possible use of AJB as a CoQ10 substitute following depletion as a result of statin therapy. We tested the effects of a statin and the resulting depletion of CoQ10 on plasma and liver lipids, erythrocyte Na efflux channels, and platelet aggregation to investigate the repletion effects of dietary CoQ10 or AJB on these parameters and antioxidation status in guinea pigs.
Materials and Methods
Animals and diets
This study was approved by the Laboratory Animal Care Committee of Jeju National University, and the animals were maintained in accordance with the Guidelines for the Care and use of Laboratory Animals of the University.
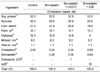
Forty 6-week-old guinea pigs (Orient Bio Co Ltd, Gapyung, Korea) were divided into four groups and fed the following diets: 0.04% cholesterol-based control diet; control diet plus 0.05% simvastatin (30 mg/kg body weight [BW]); simvastatin plus 1% CoQ10 (600 mg/kg BW); and simvastatin plus 10% AJB leave powder. The doses of AJB (Halla mountain), CoQ10 (Yunjin Pharm Co, Seoul, South Korea), and simvastatin (Choongwae Phama Co, Seoul, South Korea) are shown in Table 1. The diet was pelletized with assistance from the Korea Food Research Institute. Guinea pigs had free access to water and were housed individually cages in a room maintained at 20-25℃ with a 12-hour dark-light cycle. Blood samples were obtained by cardiac puncture into heparinized vacuum tubes after 4 weeks of ad libitum feeding, and whole blood platelet aggregation and RBC Na efflux were assessed with fresh blood. Platelet rich plasma (PRP), plasma, and liver samples were stored at -70℃ for later assays.
Whole blood platelet aggregation
Platelet aggregation was measured using a Chronolog Whole Blood Aggregometor (model 500-Ca; Havertown, PA, USA). Fresh whole blood was diluted with isotonic saline (1:4) to produce a platelet concentration of approximately 200,000 platelets/µl. Adenosine diphosphate (ADP; 2 µM; Chronolog) was added to initiate aggregation, and three impedance change readings were averaged for each guinea pig to determine the maximum aggregation and initial slope. The principle is based on the increase in impedance (Ω) across two platinum electrodes as platelet aggregation proceeds.
Plasma and liver lipid assays
Plasma total cholesterol, high-density lipoprotein (HDL)-cholesterol, triglycerides, and glucose were assayed using enzymatic kits (Asan Pharmaceuticals, Seoul, South Korea). Ten µl of plasma was used for the total cholesterol, triglyceride, and glucose assays. A 200 µl aliquot of plasma was incubated with dextran sulfate to precipitate apo B containing lipoprotein, and 50 µl of the supernatant was used for the HDL-cholesterol assay.
Liver extraction solvents were supplied by Merck (Darmstadt, Germany). Liver lipids were extracted using a modified Folch method [26]. One g of liver tissue was homogenized for 5 min in 6 ml of Folch solution [chloroform (2): methanol (1)] and 2 ml H2O. After centrifugation for 10 min, the lower phase containing the liver lipids was separated. The lower phase of the lipid fractions was assayed using enzymatic kits (Asan Pharmaceuticals) after treatment with Triton X-100:chloroform (25 µl: 475 µl) for total cholesterol or with methanol for triglycerides.
Na efflux channels
RBC preparation
Chemicals for media that included ouabain, furosemide, and morpholinopropane sulfonic acid (MOPS) were purchased from Sigma Chemical Co. (St. Louis, MO, USA). Blood was centrifuged at 1,000 × g for 10 minutes, and the plasma and buffy coat were removed. RBCs were washed five times with a cold isotonic washing solution (150 mM choline chloride, 10 mM Tris-4 MOPS, pH 7.4 at 4℃), and centrifuged at 1,000 × g for 5 minutes after each wash. The RBC pellet was resuspended in a choline chloride wash to produce a hematocrit (Hct) of 40-50%. A 50 µl aliquot of the RBC suspension was added to 5 ml of 0.02% acationox (a metal free detergent, Scientific Products, McGraw Park, IL, USA) to determine intracellular Na concentrations.
Na efflux
Four ml of the RBC suspension was added to 40 ml of MgCl2 medium with and without 1 mM ouabain (70 mM MgCl2, 10 mM KCl, 85 mM sucrose, 10 mM glucose, 10 mM Tris MOPS pH 7.4 at 37℃) to determine Na efflux via Na-K ATPase activity. Two ml of the RBC suspension was added to 40 ml choline chloride medium with and without 1 mM furosemide (150 mM choline chloride, 10 mM glucose, 1 mM ouabain, 10m Tris-MOPS pH 7.4 at 37℃) to determine Na efflux via Na-K co-transport. The RBCs in each medium were mixed and aliquoted into 12 tubes. Duplicate tubes were transferred to an ice bath after a 37℃ incubation in a shaking water bath for 0, 2, 4, 6, 8, and 10 minutes to measure Na-K ATPase and 0, 10, 20, 30, 40, and 50 minutes to measure Na-K co-transport. The tubes were centrifuged at 1,000 × g for 5 minutes, and the supernatant was removed to measure Na concentrations using an atomic absorption spectrophotometer (Shimadzu model AA6701F, Tokyo, Japan) [27].
Liver and PRP thiobarbituric acid reactive substance (TBARS) production
PRP was obtained after centrifuging whole blood at 300 × g for 10 minutes. PRP and liver TBARS production were measured with a method modified from Buege and Aust (1978). TBARS was measured with a spectrophotometer at 532 nm. Liver TBARS was measured using a nonTBA treated as a blank.
Glutamic-pyruvic transaminase (GPT) and glutamic-oxaloacetic transaminase (GOT)
Plasma GPT and GOT were measured with a spectrophotometric diagnostic kit purchased from Asan Pharmaceutical. The absorbance was read at 505 nM using a spectrophotometer, and results are expressed as IU/l.
Statistical analysis
Values were analyzed using the SAS software package (SAS, 1994). Analyses of variance were conducted in a completely randomized block design. Duncan's multiple-range test was applied to compare individual means when the F-value was significant. A P < 0.05 was considered significant.
Results
Body weights and plasma and liver lipids
Final body and liver weights were not different among the groups (Table 2). Plasma total cholesterol decreased in the statin groups compared with that in the control (P < 0.01) but no difference in HDL-cholesterol was observed among the groups. Plasma triglycerides tended to decrease in all statin groups compared with that in the control, but the difference was not significant. Liver total cholesterol was not different among the groups. Liver triglycerides decreased in all statin groups and a significant difference was observed between the control and statin plus CoQ10 group (P < 0.05).
Whole blood platelet aggregation
Maximum platelet aggregation tended to increase in the statin groups, and the initial slope tended to increase in the statin plus CoQ10 group, but no differences were observed between any two groups (Fig. 1).
Na efflux channels
The assessment of Na efflux channels is shown in Fig. 2. No difference in intracellular Na was observed among the groups. RBC Na efflux through Na-K ATPase increased significantly in the statin only group but decreased in the statin plus CoQ10 group (P < 0.05). Na efflux through Na-K co-transport increased in all statin groups compared with that in the control, (P < 0.05). Total Na efflux increased significantly in statin only group and decreased in the statin plus CoQ10 group (P < 0.05). Total Na efflux tended to match that in the major Na-K ATPase efflux channels.
Liver and PRP TBARS production
TBARS production in PRP decreased in the statin plus CoQ10 group compared with that in the control (Fig. 3). Liver TBARS production tended to decrease in the statin plus CoQ10 group, but the difference was not significant.
Plasma GOT and GPT
Plasma GOT and GPT levels are shown in Fig. 4. Plasma GOT increased in the statin and statin plus AJB groups but decreased in the statin plus CoQ10 group (P < 0.05). Plasma GPT also increased significantly in the statin only group compared with that in the control and statin plus CoQ 10 groups (P < 0.05).
Discussion
The hypochoelsterolmic effects of statins have been reported in human and animal studies. Fluvastatin (80 mg daily for 8 weeks) decreases LDL cholesterol by 35% in patients with type II hypercholesterolemia [28]. Saito et al. [29] reported that 1-40 mg rosuvastatin daily shows a linear response for reducing total cholesterol and apolipoprotein B in patients with hypercholesterolemia. Fluvastatin (3.5 mg/kg BW) decreases plasma total cholesterol and triglycerides in mice [30], and lovastatin (5 mg/kg BW) or pravastatin (2.5 mg/kg BW) reduces plasma cholesterol by 36% and 30%, respectively, along with decreases in HMG CoA reductase by 50% and 41% in chow-fed dogs [31]. In contrast, Sawada et al. [32] reported that pravastatin (1-100 mg/kg BW) increases serum cholesterol levels and dose dependently decreases serum triglyceride levels in hamsters. In rat studies, simvastatin (2 mg/kg BW) significantly increases plasma total cholesterol [33] but a high dose of simvastatin (30 mg/kg BW) in rats does not decrease plasma total cholesterol [34] In the present study, 30 mg/kg BW simvastatin decreased plasma cholesterol levels without affecting liver total cholesterol in guinea pigs, suggesting a species difference in the cholesterol and lipoprotein metabolic pathway. Approximately 65% of total cholesterol in humans is endogenously synthesized in extrahepatic tissues [35]. Fernandez [36] observed that guinea pigs synthesize moderate amounts of hepatic cholesterol, as in humans, whereas the major site of cholesterol synthesis in rats is the liver. Guinea pigs, unlike rats, carry most cholesterol in low-density lipoprotein (LDL), and upregulating the LDL receptor with statins is another way to lower cholesterol in humans and guinea pigs [36]. In the present study, the statin tended to decrease plasma and liver triglycerides, and the statin plus CoQ10 (600 mg/kg BW) treatment further decreased plasma total cholesterol and plasma and liver triglycerides, suggesting that CoQ10 potentiated the hypocholesterolemic and hypolipidemic effects of the statin. CoQ10 (15 mg/kg BW) at the same dose as a statin does not affect plasma and liver cholesterol or triglycerides in rats [34]. Simvastatin plus green tea in Kim's study [34] lowered total liver cholesterol and triglycerides, but a statin plus AJB in the present study did not affect plasma or liver lipid levels.
Statins may have a platelet aggregation function through their action on cholesterol metabolism and membrane lipids, as platelet hypersensitivity is associated with hypercholesterolemia. Atorvastatin decreases platelet cholesterol content and potentiates the action of aspirin to deactivate platelets in patients with hypercholesterolemia [17]. Fluvastatin dose-dependently inhibits platelet aggregation and decreases platelet-derived nitric oxide release in vitro [37]. Simvastatin reduces platelet adhesion to endocardium in human heart tissue and arterial segment fibrillation in vitro [38]. Despite these reports, simvastatin tended to increase maximum platelet aggregation in guinea pigs in vivo in the present study. In our previous studies with rats, low and high dose simvastatin did not affect platelet aggregation in vivo [33,34]. Depletion of antioxidants may be another factor associated with platelet activation. Antioxidants inhibit cyclooxygenases and decrease platelet thromboxane levels, which affect platelet activation and platelet responses to stimulation factors such as ADP, thrombin, and collagen [15]. Reduced CoQ10 improves platelet mitochondrial function and protects platelets from oxidative stress which, in turn, results in platelet aggregation and adhesion [16]. In the present study, CoQ10 and AJB tended to attenuate maximum platelet aggregation in the statin-treated guinea pigs, but CoQ10 may cause increased platelet sensitivity considering the steep initial slope.
Atorvastatin decreases RBC-membrane cholesterol content by decreasing the cholesterol/phospholipid ratio resulting in increases membrane fluidity with increased Na-K ATPase in guinea pigs [18]. Cholesterol content of membranes is one of determining factors of membrane fluidity. Higher concentrations of membrane cholesterol and lower Na-K ATPase activity are observed in RBCs of patients with hyperlipidemia, and pravastatin reverses or lessens this condition independent of its cholesterol-lowering effect [39]. In the present study, the statin decreased plasma total cholesterol and increased Na-K ATPase activity, which agreed with these results. However, the statin plus CoQ10 group showed further deceased plasma total cholesterol and suppressed Na-K ATPase channel activity. CoQ10 in antibiotic-treated rats recovers the reduced brush border Na-K ATPase activity and alleviates the nephrotoxicity of the antibiotic [40]. In our study, the statin also increased Na-K co-transport and Na passive transport by increasing total Na efflux. The observation that total Na efflux increased through Na channels with a higher intracellular Na in statin-treated animals is difficult to explain. AJB has strong antioxidant potency due to total polyphenol content of 21-72 mg equivalents gallic acid/g [25]. But, AJB did not favorably effect TBARS production or plasma GPT and GOT.
In conclusion, simvastatin decreased plasma cholesterol in guinea pigs, which is not observed in rats. CoQ10 seemed to potentiate the hypocholesterolemic effect of the statin and further decreased plasma cholesterol levels. Statins are analogues of HMG coA reductase and inhibit CoQ10 and cholesterol synthesis. Therefore, CoQ10 supplementation is recommended for patients undergoing statin therapy for proper electron transport system function. Exogenous CoQ10 may play roles in negative feedback of the cholesterol biosynthetic pathway. CoQ10 also effectively decreased plasma and liver triglycerides in guinea pigs, potentiating the hypolipidemic effect of the statin. Despite reports that lower plasma cholesterol levels are related with higher Na-K ATPase activity, the present study showed lower plasma cholesterol with lower RBC Na-K ATPase activity in CoQ10-treated guinea pigs, which may be explained by differences in methodology. Na-K ATPase activity in the present study was determined by Na efflux through this channel. Despite its triterpenoid content and structural similarity to CoQ10, AJB did not show cholesterol lowering, liver protecting, or antioxidant effects.





 XML Download
XML Download