

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Zinc plays important roles as an integral part or coenzyme of many enzymes including synthesis and metabolism of proteins and nucleic acids. Therefore, zinc is important for normal growth and development of humans particularly early in life. Zinc has been classified by the WHO [1] as a "problem" nutrient in complementary feeding as one of micronutrients for which requirements are often not met without supplementation in breast-fed infants starting at about six months of age.
Human milk (HM) is the ideal food for normal growth and development of infants [2], and the WHO and UNICEF [1,3] recommend that it should be given exclusively to infants for the first six months of life, and with complementary foods for up to two years of age or beyond. When breast-feeding is impossible, however, mothers must use casein-based formula (CBF). Soy-based formula (SBF) are used as a substitute for CBF in infants with lactose intolerance, cow's-milk-protein allergy or diarrhea [4]. In Korea, there are two types of commercially available SBFs, containing "soy milk" that is prepared by grinding soybeans followed by removing insoluble components or "isolate-soy protein" that is regularly used in Europe and the United States [4]. Reports are unavailable on zinc content in SBFs and zinc status of infants receiving SBFs in Korea.
The purpose of our study was to analyze zinc content in commercially available SBFs together with CBFs and HM, and to monitor zinc status and the growth of infants who were fed HM, CBF, or SBF in the first 36 months of life.
Materials and Methods
Subjects and study design
This study was approved by the Institutional Review Boards for human use of Chungbuk National University Hospital (Cheongju, Korea) and the University of Alabama at Birmingham (Birmingham, USA). After the purpose of the study was explained, mothers gave informed consent. The study was conducted from 2001 to 2006. The protocol and subjects were identical to those previously published [4]. Healthy women [n = 51, mean age of 29.6 (± 3.2, SD) years old] were recruited in the third trimester by advertisements at local prenatal care programs and maternity hospitals. They had similar socioeconomic and educational backgrounds without a history of serious disease. They delivered a healthy full-term infant at a mean gestation of 39.1 (± 1.5) weeks after uneventful pregnancy with the overall mean birth weight of 3,345 (± 459) g. Before delivery, mothers selected a feeding method from three options (HM, CBF or SBF). Mother-infant pairs visited a pediatric clinic at the University Hospital at ages 1, 2, 4, 5, 6, 12, 18, 24, and 36 months, where anthropometric data, blood and HM sample and milk/food intake history were collected at various points in the first 36 months of life as reported previously [5]. Weight and height of infants were measured by experienced nurses using an infant automatic scale (Atom, Tokyo, Japan) and a Harpenden infant stadiometer (Holtain, Crymych, UK).
Infant formulas
Dr. Chung's Co. (Cheongju, Korea) provided SBF that was offered free of charge to the SBF group. The composition of SBF (contained > 85% of "soy milk") was designed by the guidance of Codex [6] and approved as an infant formula by Korea Food and Drug Administration. The CBF group was asked to purchase any one of commercial formulas at local stores. Although mothers in the CBF and SBF groups preferred to supplement with HM, they were asked to mix-feed only for the first two weeks of lactation. All mothers were asked to adhere to the feeding method of their choice for the first five months and allowed to introduce other foods thereafter [5].
Sample collection and handling
Mothers in the HM group collected milk (-10 ml) by manual expression directly into tubes before infant feeding for the first six months of lactation. Infant blood was collected at 5, 12 and 36 months of age, and serum was separated within one hour of collection [7]. Milk and blood sampling was not always successful from all subjects each time, and samples were stored at -70℃ until analyses. A total of 24 formulas [15 CBF (powder form) and nine SBF (7 "ready to feed" and 2 powder form)] were purchased at local stores and were prepared with distilled-deionized water for zinc analysis based on manufacturers' instructions.
Assessment of dietary zinc intake of infants
Dietary zinc intakes were assessed in 1, 2, 4, 5, 6, 9, 12, 18, 24 and 36 months of life from each subject. To measure HM intake, infant was weighed before and after each feeding using an electronic digital balance (AD-15T, CAS, Seoul, Korea). To keep 24-hour HM intake records, mothers received detailed instructions for weighing procedures. At 9 and 12 months, HM intake was estimated by the nursing frequency with the mean milk volume per feeding, because it was impossible to weigh due to the limit of the balance. The mean milk volume per each feeding (105 mL) was calculated based on daily total milk intake divided by nursing frequency in 20 infants at 5 and 6 months of age. After the solid food introduction, 24-hour dietary records were kept. In the CBF and SBF groups, intakes of formulas and solid foods were recorded for two days before each clinic visit. Zinc intake from solid foods was calculated using the nutrient database in the Recommended Dietary Allowances for Koreans [8].
Zinc analysis
Serum zinc concentration was determined by the flame-atomic-absorption spectrophotometry [7], and zinc content in HM and formulas were measured by the inductively-coupled-plasma mass spectrometry [9]. The maximum precautions were taken to avoid any zinc contamination during sample collection and handling process.
Statistical analysis
The results are presented as mean (± SD) when appropriate. The differences in the means between the groups were tested by ANOVA. When the differences were significant, Tukey's post-hoc test was used to compare individual means of the groups. Pearson correlation coefficient was used to evaluate the correlations between serum zinc concentrations and zinc intakes or HM zinc contents. All analyses were done with the SAS software (Version 8.2; SAS Institute Inc., Cary, NC, USA). The P < 0.05 was considered significant.
Results
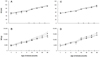
The mothers' selection of feeding methods included HM (n = 20; 8 females/12 males), CBF (n = 12; 5/7) and SBF (n = 19; 13/6). Infant growth was similar to that established for healthy Korean infants (means of height and weight were around 50th percentile of the growth standard [10]), even though there were significant differences at certain time points (Fig. 1). Only at the first month of age, the means were below the 50th percentile of the Korean standard [10], probably because our 4-week old infants at the first clinical visit had to be compared with the infants of age categorized as 1-2 months in the standard. This inevitably classified our infants below the 50th percentiles of the standard. Total energy intakes based on milk or formulas and solid foods combined were similar in all groups except at 36 months of age (Fig. 2).
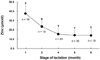
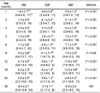
Human milk zinc concentrations declined as lactation progressed (Fig. 3). The mean zinc concentrations were 37.5, 23.5, 15.4, 14.2, and 14.0 µmol/l at 1, 2, 4, 5, and 6 months of age, respectively. Zinc concentrations in CBFs and SBFs are shown in Table 1 and these were markedly higher than HM (Fig. 3). All formulas tested in this study had higher zinc contents than those claimed by the manufacturers.
Table 2 shows calculated total zinc intakes based on HM or formulas intakes through five months of age and also based on food intakes after the introduction of solid foods until 36 months. In the first six months, infants in the HM group consistently had the lowest zinc intake among the groups, and in the first 24 months, infants in the SBF group had the highest zinc intake than the other two groups, whereas such a difference disappeared at 36 months.
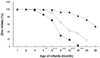
Fig. 4 shows the percentages of zinc intake of total zinc intake from HM or formulas. Mothers in the SBF group continued to feed SBF until 36 months of age, probably because formulas were offered at free of charge. Even though infants in the SBF group had a higher intake of zinc compared to those in the other two groups as shown in Table 2, more than half of zinc intake was from formulas.
Serum zinc concentrations at 5, 12 and 36 months of age are shown in Talbe 3. Although there were no difference in serum zinc at the first two time points, the mean serum zinc in the CBF group was highest followed by the SBF group, and serum zinc was lowest in the HM group at 36 months (P < 0.05, ANOVA), although the difference was small. At five months of age, six (12.8%) of 48 infants had serum zinc below the general normal cutoff of 9.9 µmol/l [11,12]. At 36 months, four (9.8%) of 41 children had such a low value, and three of these were from the HM group, although total zinc intake was not significantly different in all groups (Table 2).
There was a significant positive correlation between HM and serum zinc concentrations in the HM group at five months (n = 19, r = 0.50, P < 0.05), whereas no such associations were observed between zinc intake and serum zinc in all groups at 5, 12 and 36 months of age.
Discussion
In this study, we found that the infant growth corresponded to the normal of Korean infants and the means of height and weight were around 50th percentile of Korean growth standard in all three groups [10]. Our findings are similar to those by others [13-15] who reported a similar growth in infants given HM or different types of formulas. Although we observed significant differences in height and weight at several time points in 36 months, it appears that those may not be physiologically meaningful, since the differences and sample size were small (Fig. 1). Height and weight at 36 months of age seem to be different among the groups, probably because energy intakes (not zinc intakes) were significantly different, although we do not know the reason for the difference. Although there were infants with low serum zinc concentrations, no clinical signs of zinc deficiency were found, and their growth was around the 50th percentiles of the growth standard. Therefore, it is unlikely that these infants had inadequate zinc status.
Human milk zinc concentrations declined as lactation progressed (Fig. 3). The decline in HM zinc overtime has been well established, and there are many reports from various parts of the world [16-24]. Although the mechanism of the decline is unknown, it is possible that milk zinc values are influenced by the changes in the amount of its binding protein(s) during lactation, which may enhance zinc absorption in the neonatal period [25]. However, to our knowledge, the possible changes of such a zinc-binding protein during the course of human lactation have not been elucidated.
All formulas tested in this study had higher zinc contents than those claimed by the manufacturers, and zinc contents were higher in SBFs than in CMFs. The safe and optimal range of zinc intake is narrow unlike water-soluble vitamins, such as folate [4]. It is unknown as to whether there is any adverse effect of the long-term high zinc intake early in life.
Serum zinc concentrations at 5 and 12 months were similar in all groups (Table 3), whereas those in the CBF group were higher at 36-month old. Ohtake et al. [26] found in Japan that serum zinc of exclusively breast-fed infants remained essentially the same up to the age of three months, although HM zinc concentrations decline markedly during the same period. Despite the time point difference for the measurement of serum zinc, the concentrations reported by Ohtake et al. [26] and ours are similar, suggesting that serum zinc in those fed HM are constant early in life. In contrast to our data, Craig et al. [27] in the United States reported that plasma zinc were higher in infants fed CBF compared to those fed SBF at 3-4 months of age. Furthermore, Hambidge et al. [28] in the United States reported breast-fed infants had higher plasma zinc than those fed CBF at six months of age.
Based on our data, it is reasonable to hypothesize that zinc bioavailability is different between HM, CBF and SBF, considering similar serum zinc concentrations in all groups despite the fact that total zinc intake in the HM group was always lowest (first 6 months), and zinc intake in the SBF was highest among the groups. Using HM and formulas extrinsically labeled with radioactive zinc chloride (65Zn) and a whole-body counter, Sandström et al. [29] reported that zinc absorption in HM was 41%, cow's milk 28%, CBF 31% and SBF 22% in young healthy men, indicating that zinc in HM was about twice available compared to SBF. By measuring plasma zinc after an oral zinc dose (25 mg) together with HM, CBF or SBF in young healthy women, Casey et al. [30] reported that plasma zinc area-under-the-curve responses over three hours were 201, 57 and 34 for HM, CBF and SBF, respectively, indicating that HM zinc was about six times more available than SBF zinc. Collectively, we suggest that the reason why serum zinc concentrations were similar despite that HM zinc content was lower than CBF or SBF is due to different zinc bioavailability.
The strength of our study is that we followed zinc intake for the first 36 months of life. This is, to our knowledge, one of the longest for such a study. The weaknesses include that; 1) the total number of mother-infant pairs was small; therefore, the overall statistical power was small to draw firm conclusions; and 2) we offered the SBF free of charge; therefore, the feeding selection might have been biased due to economic reasons; and 3) the assessment of zinc intake based on 24-hour recall has a limitation in its accuracy because of the problems in the "recall" method; the accuracy of the amount of foods; and the availability of dependable and accurate zinc data in every food item consumed by our subjects.
In summary, we found that infants who were fed HM, CBF or SBF has normal growth up to three years of age, despite the fact that HM contained the lowest zinc concentration followed by CBF, then SBF. This could be explained by the different zinc bioavailability among HM and formulas. Zinc contents in both CBF and SBF were higher than those claimed by manufacturers, and careful formulation should be practiced.


 XML Download
XML Download