

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Lifestyle-related diseases, particularly diabetes, are rapidly increasing in advanced countries because of a change in lifestyle and social environment [1]. In Japan, the number of people suffering from diabetes is estimated to be approximately 22.1 million, including those with suspected diabetes, and this value is predicted to increase in the future [2]. Over 95% of the cases are type 2 diabetes, a disease that is exacerbated by excessive dietary intake, lack of exercise, and increased stress [3]. It is clear that type 2 diabetes, which is accompanied by obesity and visceral fat accumulation, has a high risk of being associated with dyslipidemia and hypertension. While type 2 diabetes can be prevented by healthy diets and adequate exercise, the number of diabetics is increasing at present because of the difficulty in maintaining healthy diets or adequate exercise.
Salacia, which has been traditionally used in Indian Ayurvedic medicine, is effective for the prevention and treatment of diabetes [4]. The active ingredients are α-glucosidase inhibitors such as salasinol [5,6] and kotakanol [7]. These substances inhibit the breakdown of oligosaccharides and polysaccharides into monosaccharides by competitive inhibition of α-glucosidase activity within the lumen of the intestinal tract, which inhibits the rapid increase of plasma glucose after meals [8]. Diabetes is often associated with visceral fat accumulation, dyslipidemia, and hypertension [9,10]. Diabetics with these symptoms use different medicines for the treatment of each symptom. This gives rise to many treatment problems because of the synergistic side effects of the numerous medicines used [3]. For the prevention of diabetes, it is important to improve not only plasma glucose levels but to also decrease visceral fat accumulation, plasma lipid levels, and blood pressure levels. Salacia was reported to improve obesity and decrease triglyceride and cholesterol levels in mice and rats [11,12]. However, not much information on these effects in humans, except for a report on the improvement of plasma glucose levels, is available [8].
The innate immune system plays an essential role in the maintenance of animal health and the prevention of various diseases. The appropriate activation of macrophages plays a central role in innate immunity and functions not only for defense against infections but also for the maintenance of homeostasis (such as the elimination of foreign substances and metabolic control) [13]. We identified a lipopolysaccharide (LPS) (molecular weight approximately 5 kD) derived from a symbiotic Gram-negative bacteria, Pantea agglomerans [14]. This LPS was capable of activating macrophages in a water extract of wheat flour [15] and was designated IP-PA1, which is an abbreviation of "immune potentiator from P. agglomerans" [13]. Under certain limited conditions, LPS may act as an endotoxin, causing severe systemic inflammation, but more commonly, it has beneficial effects. LPS functions that have been recently discovered include the regulation of intestinal homeostasis, such as preventing enteric infectious diseases or the regulation of enteric immunity through interactions with gut-associated lymphoid tissue [16,17], modulation of proliferation and differentiation of the epithelial lineages [18], and regulation of angiogenesis [19] by oral administration. Thus, LPS is now recognized as an exohormone rather than simply an endotoxin [20].
It has been demonstrated that several foods contain Gram-negative bacteria or LPS. P. agglomerans is found not only in wheat but also in other food plants, such as rice [21], sweet potatoes [22], apples, and pears [23]. Moreover, it has been demonstrated that growth of P. agglomerans is mandatory for the fermentation of rye sourdough because it produces and provides folicacid to Lactobacillus. Considering this information and the long history of human intake, the bacteria P. agglomerans is believed to be nonpathogenic. In addition, in Europe, live P. agglomerans is used as a biocontrol agent for preventing fungal spoilage of fruit [24]. This suggests that IP-PA1 is a safe substance, and this has been confirmed with a conventional oral-administration safety test [13].
Previous studies in animals and human clinical trials reported suppressive effects of IP-PA1 on IgE-dependent allergies and an analgesic effect on the acetic acid writhing test [13]. In addition, IP-PA1 was also reported to delay the occurrence of type 1 diabetes in mice [25] and decrease low-density lipoprotein (LDL) levels in familial hyperlipidemia [26]. However, it is not yet clear whether IP-PA1 is able to suppress type 2 diabetes. This is because the etiology and therapeutic approaches for diabetics are quite different for type 1 and type 2 diabetes. Also, it is not yet clear whether IP-PA1 improves diabetes associated with dyslipidemia. Thus, in this study, a tea (SI tea) was prepared that combined IP-PA1 (a regulator of immunity) and Salacia (an inhibitor of α-glucosidase), with the expectation that a beneficial effect would be observed in cases of diabetes and dyslipidemia. SI tea was first tested to determine whether it decreased the plasma glucose in KK-Ay/TaJcl mice (type 2 diabetes model mice). It was then tested to determine if it improved HbA1c values, blood glucose values, or LDL values in blood lipids of humans. This study used a randomized and double-blind design. Subjects had a routine general diet and test tea 2 times/day.
Subjects and Methods
Preparation of a mixture of Salacia and IP-PA1 (SI tea)
Salacia oblonga (Salacia) tea was prepared by Takama Co., Ltd, Japan, and the fermented flour containing 1% IP-PA1 was prepared by Macrophi Inc., Japan. IP-PA1 is a bacterial LPS that is derived from P. agglomerans. SI tea was a combination of Salacia tea, fermented flour, and vitamins. The C vitamin and B-group vitamins were premixed (B1, 0.32 mg/ml; B2, 0.27 mg/ml; B6, 0.28 mg/ml; B12, 0.75 µg/ml; B3, 1.63 mg/ml; B5, 0.96 mg/ml; and C, 7.5 mg/ml). The amount of vitamin premix was not expected to have any effect by itself on diabetes and hyperlipidemia [27,28]. In this study, 1 g of SI tea containing 20 mg/g of fermented flour extract (200 µg/g as IP-PA1) was used by dissolving in 100 ml of ambient or hot water. The control was Salacia tea without the fermented flour extract (Table 1).
Animal experiments
Five-week-old male KK-Ay/TaJcl mice were obtained from CLEA Japan, Inc. (Tokyo, Japan), and the experiments lasted for 12 weeks after 1 week of acclimatization. The mice were maintained in a temperature-controlled room at 24 ± 2℃ and 50%-70% humidity with a 12-h light cycle (light from 06:00 to 18:00). The mice were housed (1 per cage), and had access to tap water and laboratory food ad libitum (CE-2; CLEA Japan, Inc.). The mice were divided into three groups: distilled water (DW; n = 10), Salacia tea (control; n = 10), and SI tea (n = 11). The oral daily dose administered for IP-PA1 was 10 µg/kg body weight and for Salacia was 3 mg/kg body weight, accomplished by drinking SI tea for 12 weeks. Body weight and fasting plasma glucose (FPG) levels were measured every week during the course of the study for 12 weeks. FPG was measured after an overnight fast of at least 10 hours. Mice were immobilized with a stereotaxic apparatus. Blood glucose levels were determined by measuring the absorbance using an Accu-Chek Aviva (Roche). This study was approved by the Laboratory Animal Committee of Kagawa University; the mice were maintained in accordance with the Guide for Animal Experiments at Kagawa University.
Clinical study subjects
Forty-seven subjects (age range, 40-69 years) from a clinic in Kagawa participated in this study. The high-plasma glucose (HG) group consisted of 14 subjects whose FPG levels were 100-125 mg/dl; the hyperlipidemia (HL) group consisted of 33 subjects whose triglyceride (TG) levels were higher than 150 mg/dl, or whose LDL levels were higher than 120 mg/dl, or whose HDL levels were lower than 40 mg/dl (Table 2). This study was randomized in each group, and conducted using a double-blinded design. Of these, 3 subjects being treated for hyperlipidemia or hypertension were excluded from the study because of their poor physical condition or deconditioning during the intake period. The study protocol was approved by the Ethics Committee of the Non-profit Organization, Linking Setouchi Innate Immune Network, and was carried out in accordance with the principles of the Declaration of Helsinki. Procedures were carefully explained to the participants, and written informed consent was obtained from them.
Study procedure
This study initiated on October 1, 2008, and continued for 60 days. It was conducted by a double-blinded method, randomized by envelopes. Subjects ingested the routine general diet and test tea 2 times/day, and their intake time and physical conditions were recorded each day. To measure glucose metabolism markers (FPG and HbA1c) and lipid metabolism markers (TG, LDL, and HDL), blood samples were collected on days 0, 30, and 60. Subjects fasted after 22:00 on days before blood collection.
Statistical analysis
Data are expressed as mean ± SD. Statistical analyses were performed using Excel Statistics 2008 (Microsoft, USA). In the animal experiment, differences between the DW group, the Salacia tea control group, and the SI tea group were analyzed using the Tukey-Kramer multiple comparison post tests. In a clinical trial, differences between day 0 and day 30, or day 0 and day 60, were compared using the Tukey-Kramer multiple comparison post tests. Differences with P < 0.05 were considered to be significant.
Results
The beneficial effect of SI tea on plasma glucose levels in type 2 diabetic mice
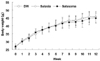
Before these clinical experiments, antidiabetic effects of SI tea were investigated using KK-Ay/TaJcl type 2 diabetic model mice. The mice had free access to tap water and laboratory food. The body weights for each group before intake were as follows: the DW group, 26.39 ± 1.07 g; the control group, 26.69 ± 1.19 g; and the SI tea group 26.84 ± 1.81 g. After 12 weeks, the body weights for each group increased in all groups as follows: the DW group, 45.64 ± 3.45 g; the control group, 45.47 ± 3.22 g; and the SI tea group 44.75 ± 3.18 g (Fig. 1). FPG levels for each group before intake were as follows: the DW group, 93.6 ± 17.6 mg/dl; the control group, 95.7 ± 18.1 mg/dl; and the SI tea group, 103.5 ± 60.9 mg/dl. After 2 weeks from the start of the experiment, FPG levels for each group were as follows: DW > control > SI tea, and this order did not change during the rest of the experiment as shown in Fig. 2. The average FPG level of each group in all periods of intake was: DW group, 118.5 ± 24.0 mg/dl; control group, 108.9 ± 24.0 mg/dl; and SI tea group, 98.5 ± 21.5 mg/dl (Fig. 2). FPG levels in DW and the control (Salacia tea) group showed a tendency to increase; while in the SI tea group, they decreased slightly. These results indicate that a combination of fermented wheat flour with IP-PA1 and Salacia effectively decreased FPG in type 2 diabetic mice more than with Salacia tea alone.
Changes in metabolism markers in humans
The above-mentioned animal data indicates that SI tea improved blood glucose levels in KK-Ay/TaJcl type 2 diabetic-model mice more than Salacia tea. Moreover, we previously found that IP-PA1 decreases LDL levels in hyperlipidemic rabbits (WHHL) [26]. We then investigated the anti-diabetic effect of SI tea in human volunteers with high-plasma glucose (HG group) or hyperlipidemia (HL group). Characteristics of each group before the clinical trial are shown in Table 3. While this study was randomized to the control or SI tea in the HG group and HL group, the body fat in the HG control group was higher than in other groups. However, the change of body fat was not significantly different for all groups.
Changes in glucose metabolism markers
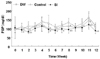
First, the effect of SI tea on the improvement of FPG levels in human HG and HL groups was examined. Fig. 3 shows the change in glucose metabolism markers over the 60-day period. FPG levels in each group before initiating the intake were as follows: the HG control group, 105.2 ± 7.6 mg/dl; the HG SI tea group, 105.4 ± 5.8 mg/dl; the HL control group, 92.3 ± 3.0 mg/dl; and the HL SI tea group, 91.8 ± 5.5 mg/dl. Sixty days after initiating the intake of teas, the FPG values were as follows: the HG control group, 98.7 ± 6.3 mg/dl; the HG SI tea group, 103.7 ± 16.2 mg/dl; the HL control group, 87.2 ± 6.2 mg/dl; and the HL SI tea group, 85.0 ± 6.7 mg/dl. Thus, the level of FPG in the SI tea group did not change. However, the FPG level of the HL group that consumed SI tea showed a significant decrease earlier than the control. HbA1c levels in each group before initiating the intake were as follows: the HG control group, 5.2% ± 0.6%; the HG SI tea group, 5.2% ± 0.3%; the HL control group, 4.9% ± 0.3%; and the HL SI tea group, 5.0% ± 0.2%. Sixty days after the intake of teas, the HbA1c values were as follows: the HG control group, 5.0% ± 0.6%; the HG SI tea group, 5.0% ± 0.4%; the HL control group, 4.9% ± 0.3%; and the HL SI tea group, 4.9% ± 0.2%. As with FPG, the level of HbA1c in the HG group was almost the same in the control and SI tea groups. In contrast, the level of HbA1c in the HL group significantly decreased after 30 days in the SI tea group. These results suggest that IP-PA1 promoted a decrease of this glucose metabolism marker when combined with Salacia tea. In addition, this combination effect of IP-PA1 with Salacia was more prominent in the HL group than in the HG group.
Changes in lipid metabolism markers
Next, we investigated the changes in lipid metabolism markers. Table 3 shows that before the experiment, the TG level in the HL control group was high, 152.5 ± 80.3 mg/dl. Also, the LDL level was high in all of groups: the HG control group, 140.0 ± 26.9 mg/dl; the HG SI tea group, 136.1 ± 29.9 mg/dl; the HL control group, 140.8 ± 31.7 mg/dl; and the HL SI tea group, 148.1 ± 32.2 mg/dl. The TG level did not change in any of the groups. However, the TG level in the HL group that consumed SI tea and Salacia tea showed a tendency to decrease (Fig. 4). The LDL level for those who consumed SI tea decreased both in the HG group and the HL group after 60 days, 122.1 ± 34.6 mg/dl and 142.1 ± 39.1 mg/dl, respectively. The HDL level significantly increased in the HG group after consuming SI tea for 30 days (58.1 ± 13.0 mg/dl). As a result of the study on TG, LDL, and HDL values, it was confirmed that LDL values, which were higher than normal levels before the trial, had decreased significantly after administration of SI tea.
Discussion
In Japan, over 95% of diabetics have type 2 diabetes. While suppressive effects of IP-PA1 on the occurrence of diabetes development in NOD type 1 diabetic-model mice have been reported [25], the effect of IP-PA1 on type 2 diabetes is still unclear. This is why we investigated the beneficial effects of SI tea on FPG levels in a type 2 diabetic mouse model (KK-Ay/TaJcl mice), which is based on a lifestyle disease. The result of body weight change was confirmed to increase in all groups, and it was not different among the groups. It was reported that there was a slight weight loss in mice and rats that were fed with Salacia [11,12]. In another study, after Salacia intake for 3 weeks, it was reported that body weight did not differ between the control and Salacia groups [29]. Thus, the addition of IP-PA1 did not induce abrupt body weight change similar to Salacia alone, and if our study was prolonged, it may have been different between the control group and the SI group. The results indicated that levels of FPG in DW and control (Salacia tea) groups gradually tended to increase but slightly decreased in the SI tea group (Fig. 2). Since FPG levels of the control Salacia tea group showed a tendency to increase, this suggests that SI tea has the potential to improve type 2 diabetes and that this effect is superior to Salacia tea alone.
Salacia tea reduces high blood glucose levels because it contains salacinol and kotalanol, both of which are inhibitors of α-glucosidase. It is known that guava polyphenol, mulberry, and Gymnema also have similar inhibitory activity against α-glucosidase but Salacia is the most effective [30]. While the antidiabetic mechanism of IP-PA1, a macrophage-activating substance, remain elusive, macrophage activation has been reported to be effective in treatment of type 1 and type 2 diabetes [31-34].
Type 1 diabetes is caused by the progressive loss of insulin-producing pancreatic β cells by inducing auto-reactive cytotoxic T lymphocytes [35]. Moreover, it has recently been demonstrated that killer T cells initiate an inflammatory cascade within the adipose tissue, and that this induces insulin resistance in type 2 diabetes [36,37]. Therefore, type 1 and type 2 diabetes are similar inflammatory diseases.
Recently, two different states of macrophages have been defined: the M1 (or classically activated) and M2 (or alternatively activated) macrophages [38]. M1-activated macrophages typically produce pro-inflammatory cytokines (tumor necrosis factor (TNF)-α, interleukin (IL)-1β). M2 macrophages increase anti-inflammatory cytokines (IL-10) and arginase 1 activity. Functionally, M2 macrophages down-regulate inflammatory responses and promote tissue repair. Adipose tissue macrophages in obesity induce an inflammatory reaction (such as TNF secretion) in cytokines, whereas macrophages in healthy adipose tissue release anti-inflammatory cytokines such as IL-10 and TGF-β [39,40]. We found an anti-inflammatory response to IP-PA1 in atopic dermatitis experiments [13]. Porta et al. [41] reported that M2 macrophages are induced by a small amount of LPS for a long period. In animal models, nicotine treatment reduces the incidence of type 1 diabetes animal models by increasing the pancreatic levels of the M2 cytokines IL-4 and IL-10 [42]. These results suggest that M2 type macrophages released IL-10 from macrophage activated by IP-PA1, suppressing the inflammatory response. Details of the mode of action for the anti-diabetic effect of IP-PA1 requires further investigation, such as the measurement of diabetes-associated markers (TNF-α, IL-1β and IL-10), insulin, and leptin.
The improvement in human plasma glucose levels is shown in Fig. 3. To examine the preventive effect on diabetes, non-diabetic subjects were chosen with high FPG levels (HG: FPG 100-125 mg/dl). The results indicate that SI tea did not change FPG levels, although it showed a tendency to reduce HbA1c levels. Type 2 diabetes is often accompanied by obesity and dyslipidemia. The most common pattern of diabetes is characterized by the secretion of TNF-α from adipose tissue because of dyslipidemia, which leads to impaired insulin sensitivity and impaired glucose tolerance (IGT) [43]. As stated above, in healthy individuals with normal body weight, macrophages are present in moderate quantities in adipose tissue, in which inflammatory signals are low or nonexistent. On the other hand, the adipose tissue macrophages in obese individuals produce pro-inflammatory cytokines and induce IGT [44]. It is suggested that macrophages are either suppressors or enhancers in the development of diabetes. However, several issues are still unclear about the mechanism that regulates the differentiation of macrophages, and the relationship between the onset of diabetes and macrophage behavior.
Our previous study showed that the serum cholesterol level in WHHL rabbits decreased with the uptake of IP-PA1 [26]. Kishino et al. [12] indicated that Salacia improves obesity and decreases plasma lipid levels by lipase inhibition in mice and rats. Thus, it was expected that herbal tea containing Salacia and IP-PA1 would improve not only plasma glucose but also serum cholesterol levels in subjects with dyslipidemia. We investigated the SI tea effects on plasma glucose levels and plasma lipid levels in a group of subjects which consisted not only of a high glucose group but also a high lipid group (TG: ≥ 150 mg/dl, or LDL: ≥ 120 mg/dl, or HDL: < 40 mg/dl). As shown in Fig. 3, significant changes in levels of FPG and HbA1c were observed in the HL group as in the HG group. Especially, the FPG level of the HL group that consumed SI tea was significantly lower than that of the HG group. In this study, the FPG level of the HL group stayed within the normal level. However, even if the FPG level is normal, Japanese people tend to develop IGT because their insulin secretion ability is lower than in other ethnic populations [45]. High IGT levels increase the risk of occurrence of diabetes and arteriosclerosis to a greater extent than high FPG levels [46,47]. Moreover, a correlation between a decrease in IGT and FPG was reported [48]. Since a significant effect of decreasing plasma glucose levels due to SI tea was observed in the HL group but not the HG group, it is believed that SI tea may be effective for IGT. This would not be obvious from the FPG values alone. SI tea significantly reduced LDL levels in the plasma lipid of both HG and HL groups. In addition, there was a significant increase in the HDL level of HG groups that consumed SI tea. LDL levels of all subjects from all groups before the experiment were high (Table 3). While in the present study, a change in obesity was not observed with Salacia (Table 3), Akase et al. [11] reported that Salacia decreased body weight and visceral fat in mice and rats. The difference in the results was most likely because of the difference between a regulated rodent model and a human experiment in which it is difficult to control food and life style.
In conclusion, SI tea not only decreased FPG levels more effectively than Salacia tea alone but it also improved LDL values. Thus, it can be anticipated that SI tea will be used as a preventive food for lifestyle-related diseases, such as diabetes, obesity, and dyslipidemia.





 XML Download
XML Download