

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Collection and assessment of usual dietary intake data in free-living populations are challenging in terms of reliability and validity [1-3]. Monitoring of usual intake requires collection of dietary intake data over a long period [4], which is not feasible in large scale population studies.
Food frequency questionnaires (FFQs) and 24-hour recall are two common approaches for collecting dietary data. Although FFQs are designed to measure long-term dietary intake, their validity highly depends on the list of food items the questionnaire as well as participants' cognitive functions [5-8]. On the other hand, 24-hour recall is convenient in collecting information about food types and amounts, but its validity is limited in estimating usual intake due to large day-to-day variations in individual dietary intake. In order to compensate for daily variations, researchers average multiple 24-hour recall or use statistical approaches [9,10].
Several statistical methods have been developed over the last two decades to address the limitations of 24-hour recall in estimating usual dietary intake of populations. Most of these methods focus on controlling the so-called within-individual variation of short-term dietary measurements. Hoffman et al. [11] compared six different statistical methods to estimate usual intake distribution. Dodd et al. [9] recently reviewed the theory of the statistical methods for estimating usual intake distribution. The authors concluded that the usual intake distribution calculated from statistical modeling approach is closer to the distribution of doubly labeled water measurement than those of FFQs and one 24-hour recall.
The Dietary Reference Intakes for Koreans (KDRIs) [12] with Estimated Average Requirements (EARs) and Tolerable Upper Intake Levels (ULs) are important references in estimating the prevalence of inadequacies in order to establish appropriate public health policies. However, interpretation depends largely on valid estimation of usual intake of the population [13,14].
In this study, we assessed nutritionally inadequate subjects based on Korean DRIs, using the Iowa State University (ISU) method, from adjusted one-day 24-hour recall data by controlling within-individual variations of subsamples. To calculate the proportion of inadequate or excessive intake, we applied Korean EARs or Korean ULs to the adjusted and unadjusted distributions of dietary intake data.
Subjects and Methods
Study subjects and design
The dietary intake data used in this study were from the 2001 KNHNS and the 2002 Korean National Nutrition Survey by Season (KNNSS), which were conducted by the Korean Ministry of Health and Welfare. The purpose of the surveys was to estimate the yearly food intake and assess health and nutritional status among Koreans. The 2001 KNHNS was a cross-sectional survey conducted in nationally representative samples between November and December of 2001 [15]. A total of 43,032 individuals from 13,200 households of 600 Primary Sampling Units (PSUs) took part in the 2001 KNHNS in one or more of four parts: Health Interview Survey, Health Behavior Survey, Health Examination Survey and Nutrition Survey.
Data collected in the Nutrition Survey were interviewer-administered one 24-hour recall of 9,968 individuals from 4,000 households of 200 PSUs. Three additional 24-hour recalls were repeated in three subsequent seasons in the 2002 KNNSS to offset seasonal variation in food intake and estimate the annual food intake of the Korean population [16]. In 2002, the subjects were selected by a rotation sampling method as depicted in Fig. 1. Briefly, the rotating sampling method for the 2002 KNNSS spring survey included 500 overlapping households of 50 PSUs out of 200 PSUs surveyed nationwide in the 2001 KNHNS. Similarly, another 500 overlapping households of 50 PSUs were made in the subsequent 2002 KNNSS summer survey. For the 2002 KNNSS fall survey, the same rotating sampling scheme was used to overlap 500 households of 50 PSUs between summer and fall surveys (Fig. 1). In this manner, individuals from 1500 households of 150 PSUs had two 24-hour recall data.
Dietary recall data of the 2001 KNHNS and the 2002 KNNSS were collected by trained interviewers from each individual at their residence using 43 food models and 281 color photographs of foods to assist in estimating portion sizes. The 6th edition of the food composition table from the National Rural Living Science Institute [15] was used to calculate nutrient values in foods. The database of the National Rural Living Science Institute consisted of 2,337 food items and 2,294 dishes [15]. Further, the processed food database containing a total 2,752 food items, including 1,250 processed foods, 690 imported foods, 553 fast foods, and 259 nutritional supplements, was used. In the end, two 24-hour recalls were collected from 3,976 individuals through the 2001 KNHNS and the 2002 KNNSS. The two-day intake data were used to estimate within-individual variance, and all of the one-day intake data of the 2001 KNHNS were used to estimate the percent of subjects with inadequate and excessive intake in reference to 2005 KDRIs.
Estimation of usual intake distribution
The X-Windows-based version of the Software for Intake Distribution Estimation (C-SIDE) (version 1.02, 1996; available from the Center for Survey Statistics and Methodology, Iowa State University, Ames, IA, USA) along with an additional guidebook were used to estimate the usual intake distribution [17-19] adjusted by within-individual variations.
A three-step process ensued to produce the results of the present study.
Within-individual variances were estimated by C-SIDE for each nutrient for gender/age subgroups using the two-day intake data derived from the 2001 KNHNS and the 2002 KNNSS.
One-day intake from the 2001 KNHNS was analyzed with C-SIDE using the within-individual variance estimated from step 1 as outer inputs in order to calculate the estimated adjusted intake distribution [20].
C-SIDE was used to estimate nutritional adequacy of the population in reference to the KDRIs.
Assessment of nutrient intakes
According to the definition of KDRIs, nutritional inadequacy of the population was assessed for individual nutrient for which Korean EARs and Korean ULs reference values had been established. For assessment of sodium intake, the WHO/FAO's Intake Goal to prevent chronic disease, i.e., less than 2000 mg/day, was used.
The usual intake distributions of ten micronutrients and three macronutrients were calculated: protein, vitamin A, vitamin C, thiamin, riboflavin, niacin, calcium, phosphorus, sodium, iron, carbohydrate, protein, and fat. The macronutrients were applied with the Atwater coefficients, calculated % energy contribution for comparison with the Korean Acceptable Macronutrient Distribution Ranges (Korean AMDR).
Statistical analysis
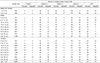
The percentage of subjects whose one day intake was inadequate or in excess in reference to the KDRIs was computed using the SAS program (version 9.1, 2002, SAS Institute, Inc., Cary, NC, USA). The prevalence of nutritional inadequacy and excess was estimated based on usual intake distributions produced by the ISU method as described above. Percentage of subjects whose intake was less than the Korean EARs, above the Korean ULs, and below and above the Korean AMDR was calculated using C-SIDE software. The ten micronutrients analyzed and compared to the Korean EARs or the Korean ULs in this study are presented based on estimates of usual intake distributions: mean, standard deviation, and intakes at the 5th, 10th, 25th, 50th, 75th, 90th and 95th percentiles.
Results
Comparison between the two distributions of the adjusted intake using the ISU method and unadjusted one-day intake is shown in Table 1. Total population includes everyone over one year of age (n = 9,960). The variances in intake distribution of all nutrients and percentage of energy source examined became smaller when adjusted for within-individual variance as compared to the one-day intake distribution. The usual intake distribution changes in vitamin C and sodium, which exhibited remarkable differences before and after adjusting, in those aged over 20 years using the 2001 KNHNS are presented as examples. Fig. 2 shows the comparison of vitamin C and sodium intake distributions before and after adjusting for within-individual variations using the ISU method. The distribution curves of the adjusted 24-hour recall data were taller and narrower than the unadjusted one 24-hour recall data. The prevalence of vitamin C inadequacy decreased to 4.9% after the adjustment compared to 32.5% when one 24-hour recall was used. Before adjustment of 24-hour recall distribution, the proportion of population with excessive sodium intake was 92.8%, however, in the adjusted 24-hour recall distribution, almost all subjects' intakes were over the Intake Goal (< 2,000 mg/day).
Prevalence of inadequate intake estimated by adjusted intake vs. one-day intake
The percentage of individuals whose daily intake was below the Korean EARs based on the adjusted data distribution using the ISU method and one-day data are compared in Table 2. In the Korean population, inadequate intake of calcium was most prominent at a rate of 73%. Inadequate intake of riboflavin (data not shown) and iron was also prevalent at rates of 41% and 24% of the population, respectively. Phosphorus (data not shown) and protein were the nutrients for which the prevalence of inadequate intake was relatively low. Most of the nutrients may be problematic for an elderly subgroup aged over 65 years compared to other gender/age groups. Overall, the prevalence of inadequate intake diminished after adjusting for within-individual variations, with the exception of calcium. Among the nutrients showing the largest changes before and after adjusting for within-individual variations, vitamins C and A exhibited differences of 28% and 27.3%, respectively.
Prevalence of excess intake estimated before and after adjusting for within-individual variations
The percentages of subjects whose intakes were above the Korean ULs for two nutrients and above the Intake Goals for sodium were compared based on adjusted intake distribution and one-day intake (Table 3).
Excessive intakes over the Korean ULs did not surface seriously for the nutrients studied in most subgroups. However, sodium intake exceeded the Intake Goal in nearly 100% of all subgroups. Interestingly, the percentage of population whose intake exceeded the upper intake levels was higher in the 1-2 years group than in the other age groups. Overall, the proportion of subjects whose intake was excessive decreased when the adjusted intake was used compared to one-day intake. Conversely, the proportion of the population whose sodium intake exceeded the Intake Goal was higher when adjusted intake was used compared to one-day intake. This is because the variance reduced through adjustment decreased the size of the population whose intake fell away from the median. In the case of sodium, however, the one-day intake of most subjects was already higher than that of the Intake Goal, and thus reduction in variance by the adjustment process reduced those whose intake fell below the Intake Goal.
Prevalence of inadequacy and excess intake of macronutrients estimated before and after adjusting for within-individual variations
The percentage of the population whose intake of macronutrients was under and over the Korean AMDR is summarized in Table 4. According to the 2001 KNHNS, carbohydrates were the primary source of energy, with 67% of daily energy derived from carbohydrates. The percentage of energy intake from carbohydrates exceeded the Korean AMDR (55-70%) in all women over 20 years of age and particularly in older women over 65 years of age, constituting 50% and 84%, respectively. Conversely, the percentage of subjects whose energy intake from fat was less than the Korean AMDR level was high in women and older women, constituting 46% and 84%, respectively. The percentage of energy from protein was approximately within the Korean AMDR.
Discussion
In the present study, we estimated the prevalence of nutrient inadequacies and excesses among Koreans compared to KDRIs before and after adjusting for within-individual variations. Importantly, we compared the estimated prevalence by one-day intake data versus by usual intake data adjusted by the ISU method. In both approaches, the intakes of calcium, iron, riboflavin, and vitamin A were inadequate, whereas intake of sodium was excessive. In addition, high intake of carbohydrates and low intake of fat were determined by calculating the energy composition ratio of macronutrients.
Inadequate intake of calcium and iron in Koreans has been reported in several studies using non-representative samples [21-23]. Inadequate intake of calcium and riboflavin has also been reported in the population survey of the Korean National Nutrition Survey (KNSS) conducted from 1969 to 1989. The trends of nutrient intake based on the KNNS for the 20-year period [24] indicated inadequate intake levels of calcium and riboflavin as well as adequate intake of thiamin, niacin, and vitamin C. Based on the 2001 KNHNS dietary survey data, the Korean Ministry of Health and Welfare reported that calcium intake was inadequate for the entire population, whereas intake levels of vitamin A and riboflavin were inadequate for the population aged over 65 years [15]. At that time, the Recommended Dietary Allowance for Koreans (Korean RDA) was used to assess the percentage of the population whose intake was inadequate (< 75% of the Korean RDA) or excessive (> 125% of the Korean RDA). Consistent with the aforementioned reports, the problematic nutrients identified in our study were the same, though the percentage of the population whose intake was at risk differed. In the present study, the adjusted intake distribution decreased the percentage of the population whose intake was below the Korean EARs by 8.8-28% compared to that assessed by one-day intake data. Only calcium demonstrated the opposite result; the percentage of the population whose intake of calcium was below the recommended increased by 3.2%. These increased proportions of inadequacies after controlling for within-individual variations have also been reported elsewhere [25,26], especially for some nutrients for which the median intake lies far below the EAR, regardless of the statistical approaches or software used.
Consistent with previous reports, Koreans in the present study consumed a higher percentage of energy from carbohydrates (67%) and a lower percentage from fat (19%) compared to the Korean AMDR. Park et al. [27] reported that the percentage of energy from carbohydrates decreased, whereas those from protein and fat increased in Korea from 1969 to 1988. They also reported that the percentages of energy intake from carbohydrates, protein, and fat were 67:19:14%, respectively, in 1988. Based on these data, we can conclude that the energy distribution of macronutrients has stabilized in Korea but remains higher than the Korean AMDR in adults. In addition, the percentage of energy derived from fat appears to have remained low for Korean adults relative to the Korean AMDR, although it has trended upward over time. Garriguet in Canada [28] reported in 2007 a composition ratio of macronutrients of 51:17:32% for carbohydrates, protein, and fat, respectively, in a study involving more than 35,000 subjects from the Canadian Community Health Survey data of 2004 using C-SIDE software.
Koreans have one of the highest rates of total 24-hour urinary sodium excretion in the world [29], and stomach cancer is the second most prevalent cancer death in Korea. In addition, approximately 30% of the adult population has hypertension [30]. Many epidemiological, clinical, and experimental studies have proposed that high intake of dietary salt is related to the prevalence of hypertension and stomach cancer [31-33]. Therefore, recommendations to decrease salt intake are common worldwide [34]. Researchers have also identified a dietary pattern that takes in a great deal of salt from food in Korea [35,36]. The KDRIs nevertheless include an Intake Goal of sodium (< 2,000 mg/day) for the prevention of chronic diseases. In this study, we also confirmed that the proportion of excessive sodium intake was unacceptably high. Excessive sodium intake in the diet of Koreans remains a serious public health concern.
Except for iron and niacin, the proportion of the population whose intake exceeded the Korean ULs was very low. Vitamin A was the only nutrient in which a small proportion of the population exceeded the Korean ULs. This result is, however, based solely on food intake, which represents one of the limitations of the present study. When food intake is combined with supplements, the proportion exceeding the Korean ULs will likely increase. It is expected that public health issues surrounding excessive intake of certain nutrients in the Korean population will soon surface.
In the present study, under-reporting or over-reporting dietary intake by the survey population could not be delineated. Goldberg criteria have been commonly used to correct the overall bias of under-reporting at the group level [37], but information that can classify individuals into three categories relative to energy expenditure was not available from the 2001 KNHNS. Another limitation of this study was that seasonal variations were not taken into account. The dietary data used in this study were collected during different seasons; therefore, it would have been appropriate to remove the effect of seasonal variation. Moreover, the ISU method was designed to take into account the sequence of observations, such as the day of the week or time of year. However, the overlapping dietary data from the 2001 KNHNS and 2002 KNNSS were merged to create two-day dietary data without considering the season, day of the week, or time of year. Through the merging process, two-day dietary data from different seasons were regarded as a single dataset to estimate within-individual variation. In spite of this limitation, the present study is one of the first studies to estimate typical nutrient intake levels among a representative Korean population and determine the prevalence of nutritional inadequacies and excesses that are associated with within-individual variation.
In this study, we confirmed that estimated prevalence of inadequate intake based on one-day intake results in over or under-estimation, since within-individual variation is not considered. In the Korean population, average intakes of calcium and riboflavin were the most inadequate, whereas sodium intake was the most excessive. Adequate dietary intakes of Koreans were observed for protein, phosphorous, and percentage energy from protein. After adjusting for within-individual variation, the magnitude of inadequacy decreased for most nutrients. Researchers interested in estimating the percentage of persons below or above a certain standard should keep in mind that one 24-hour recall could be misleading in terms of within-individual variation. To achieve an optimal state of public health in Korea, nutrients that were inadequately consumed in this study should be managed by nutritional policy and be made known in the hopes of stimulating interest regarding this topic.





 XML Download
XML Download