

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Stroke survivors often face serious swallowing difficulty, and it is reported that about 24.3-52.6% of stroke patients suffered dysphagia [1,2]. Thus, enteral nutritional supports have been used via tube feeding to those dysphagic stroke patients. However, only 37.8-43.8% showed adequate nutritional state in the stroke patients receiving enteral nutrition [3]. Dysphagia, inadequate diet intake, and increased energy requirements during recovery might increase the risk of malnutrition [4]. In addition, nutritional status influences length of hospital stay, complications, and mortality of stroke patients, thus, it is necessary to optimize nutrition management for the patients [5,6]. For the nutritional purpose, enteral nutrition showed some physiological advantages, fewer complications, and cost less than parenteral nutrition [7,8]. Moreover, recent studies revealed that enteral diet containing antioxidants had improved clinical outcomes [9].
On the other hand, quality of life in caregivers is an important issue, because caregiver-burden has been proved to affect patients' clinical outcome. For example, if the caregiver got stressed or depressed, rehabilitation of the patients was proved to be less successful [10]. If the caregivers were healthy and felt capable of providing the care, their care was proved to have positive effect on the recovery, rehabilitation and survival of patients [11,12].
Recently, various commercial enteral formulas are administered to many hospitalized or home patients. In addition, many stroke patients require enteral feeding for several years or their whole life. Thus, there are great concerns about long term use of enteral products. However, few studies have been performed to see long term effects of commercial enteral formulas. In a case of commercial formula N, it has been used over 10 years in Korea for dysphagic patients with good price, compared to other imported formulas. Therefore, we performed two separate studies, i.e. a long term trial to evaluate N's effects on the patients' health and nutritional status and their caregivers' quality of life, and another short term trial to see equality between N and another expensive formula J. For these studies, we analyzed 19 health and nutritional biomarkers. Considering the stroke causes and progress, which are related to reactive oxygen species (ROS), we also analyzed an oxidative stress biomarker, malondialdehyde (MDA), and assessed effects of the formulas on stroke progress. Finally, we investigated SCQ levels among caregivers to evaluate the benefit of enteral products for caregiver burden.
Subjects and Methods
Study subjects
This study was approved by IRB at Seoul National University Bundang Hospital (SNUBH), Sookmyung Women's University, and Seoul Veterans Hospital. We recruited outpatients who were taken care of community nurses. For a long term study, inclusion was restricted to patients, who were more than 1 year after stroke onset and had been fed a commercial enteral formula N, at least 600 kcal/day for more than 1 year. The subjects were provided enteral formula N (1,200 kcal/day) for 6 months. Previous food habits were allowed to avoid any kind of artificial effects during the experiment, if they did not exceed daily calorie requirement. Blood samples were collected before the trial and at 2, 4, and 6 months after the trial.
For a short term study, we recruited acute stroke patients within 1-3 months after the onset of stroke. Twelve patients participated in the short term intervention. We randomly divided the 12 subjects into two groups for administration of commercial enteral formula N or J (1,500-1,800 kcal/day due to calorie requirement). Formulations of the two commercial enteral formulas are described in the Table 1. Blood samples were collected before intervention and at 4, 7, and 14 day. To estimate individual daily calorie requirement, we used Harris-Benedict equation (HBE) for basic metabolic rate (BMR) and added activity factor to the BMR.
Questionnaires
Data of patients and caregivers were obtained from questionnaires including characteristics of patients and caregivers, and sense of competence questionnaire (SCQ). Following one interviewer's instruction, caregivers filled out the same questionnaires at 'before' and 'after the trial'.
We modified Scholte op Reimer et al. [13]'s SCQ and our SCQ reflected caregivers' perceived burden with 3 subscales in total 27 items (subscale 1, satisfaction with the impaired person as a recipient of care, 7 items; subscale 2, satisfaction with one's own performance as a caregiver, 12 items; subscale 3, consequences of involvement in care for the caregiver's personal life, 8 items). Each item was graded with 4-point rating scale (1, no burden; 4, the highest burden): range of total score, 27 to 108.
Analysis of nutrition- and health-related biomarkers
For biochemical analyses, each subject donated 5-10 ml of peripheral blood after an overnight fast. Whole blood samples were prepared from blood anticoagulated with ethylene diamine tetra acetic acid (EDTA) tubes (BD vacutainer, Franklin Lakes, NJ, USA). Gently inverting the EDTA tubes 8-10 times immediately after collection, we stored them in a refrigerator (0-4℃). Within 24 hrs, white blood cell (WBC), red blood cell (RBC), hemoglobin, hematocrit, platelet, mean corpuscular volume (MCV), mean corpuscular hemoglobin (MCH), and mean corpuscular hemoglobin concentration (MCHC) were analyzed in the blood samples using an automatic hematology analyzer (Hemavet 850, CDC Technology, USA). In addition, serum samples were prepared from blood samples in serum separator tubes (SST: BD vacutainer). SSTs were gently inverted 8-10 times and allowed to clot for 30 minutes in vertical position. After coagulation, they were centrifuged at 3,000 g for 10 minutes, and stored in a refrigerator. Within 24 hrs, 11 biochemical markers including albumin, total protein, transferrin, triglyceride, high density lipoprotein (HDL), low density lipoprotein (LDL), total cholesterol, homocysteine, vitamin B12, sodium, and potassium were analyzed [14-22].
Medical records, e.g. demographic data, drug usage, and complications, were obtained to assess the health condition of patients. In addition, modified rankin scale (mRS) was assessed to classify disability. The scale of mRS runs from 0-6 (0, no symptoms; 1, no significant disability; 2, slight disability; 3, moderate disability; 4, moderately severe disability; 5, severe disability; 6, dead) [23]. The mRS was diagnosed by attending physicians for acute patients or trained community nurses for chronic patients. The scale raters referred to detail guidelines of Wilson et al. [24] for elimination of diagnostic bias.
Analysis of malondialdehyde (MDA)
MDA was analyzed as MDA-thiobarbituric acid complex with HPLC/UVD [25]. In brief, standards of tetraethoxypropane (TEP: Sigma-Aldrich, Saint Louis, MO, USA) were serially diluted in 40 % ethanol everyday, and 0.06, 0.125, 0.25, 0.5, and 1.0 µmolL TEP were used for calibration. The TEP standards or 250 µl of plasma samples were treated with 25 µl of 0.2 % butylated hydroxytoluene (BHT: Sigma-Aldrich) in absolute ethanol, and followed by addition of 1 ml of 5 % trichloroacetic acid (TCA: Sigma-Aldrich). The mixtures were vortexed and centrifuged at 4,000 g for 10 min. Five hundred µl of 0.6 % thiobarbituric acid (TBA: Sigma-Aldrich) was added to the 700 µl of deproteinized supernatant. The mixtures were vortexed and incubated for 45 min at 90℃. After ice-cooling, the reaction mixtures were centrifuged at 4,000 g for 10 min. Four hundred µl of the supernatant of each sample was loaded to a HPLC-vial.
HPLC/UVD system was composed of dual Younglin SP930D pumps (Younglin, Seoul, Korea), MIDAS COOL autosampler (Spark Holland, Emmen, The Netherlands), Shimadzu SPD-10A UV/VIS Detector (Shimadzu corporation, Tokyo, Japan), XTerra C18 column (5 µm, 4.6 × 250 mm, Waters, Wexford, Ireland), and CTS30 column oven (temperature at 40℃: Younglin). Mobile phase was made of 50 mM KH2PO4/K2HPO4 buffer (pH 6.8) and methanol (58:42). Samples were analyzed with flow rate of 0.3 ml/min at 532 nm (injection volume, 200 µl)
Statistical analysis
Data were analyzed with SPSS (SPSS Inc, Chicago, IL, USA). Regression analyses were performed to study the enteral formula-induced changes in 20 biomarkers during the trials. Chi square test and Student's t-tests were used to compare the characteristics between the N- and J-treated groups. Multivariate Analysis of Variance (MANOVA) was performed to compare effects of enteral formulas, N and J, on 20 biomarkers during the intervention. Paired t-test was used to compare the differences in caregiver burden or MDA levels between before and after the interventions. Differences were considered as statistically significant at P < 0.05.
Results
Long term trial
All patients in the long term trial were men, and their characteristics are shown in Table 2. Considering mRS-score, their disability is thought to be severe. Each subject was administered with almost same drugs such as antiepileptic drugs, antihypertensive drugs, anticoagulant drugs, diuretics, antiulcerants, and expectorants during the 6 month intervention.
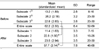
In a case of biomarker analyses, abnormalities in HDL, hemoglobin, hematocrit levels were somewhat improved, even though there wasn't any significant change in the biomarkers during the study (Table 3). Concerning normality, HDL, sodium, RBC, hemoglobin, hematocrit and transferrin levels were slightly under the normal range, while MCV and vitamin B12 levels were higher than normal range for the intervention. Other biomarkers were within normal ranges. In addition, levels of MDA, an oxidative stress marker, were somewhat increased (before, 0.24 ± 0.02; after, 0.26 ± 0.02 µM, P > 0.05).
Concerning SCQ among the caregivers, entire burden was significantly decreased due to the administration of the N. In addition, the subscale 2 score (satisfaction with one's own performance as a caregiver) was also significantly decreased (Table 4).
Short term trial
Before performing a short term trial, we confirmed that there were no characteristic differences between two groups, who were ready to formula N or J (Table 2). One male patient among the N-treated group had severe stomach problems for several days during the trial, thus, his data of biomarkers were excluded. The characteristic differences between the N and J groups were not significant without him.
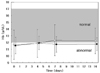
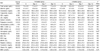
In the N-treated group, 19 biomarker levels were not significantly different between before and after intervention. Nutritional status from 19 biomarkers was maintained in normal during the study, except triglyceride, RBC, hemoglobin and hematocrit. Similarly, nutritional status of J-treated group was generally normal except triglyceride, HDL, RBC, hemoglobin, hematocrit, and vitamin B12 levels during the intervention. Finally, there was no significant difference in most of the analyzed biomarkers between the 2 groups (Table 5). Only hemoglobin levels were significantly improved more in the N-treated group than the J-treated group (P = 0.02, Table 5; Fig. 1).
We found that MDA levels were decreased for the treatment (before, 0.22 ± 0.03; after, 0.19 ± 0.02 µM, 0.05 < P < 0.1). However, there was no significant difference between effects of the N and J groups on MDA levels.
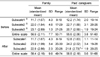
In case of SCQ analysis for their caregivers, we found that there was no significant difference in entire scale scores or subscale scores between the N and J groups. When we divided caregivers into two groups, i.e. family members and paid caregivers, there was a significant increase in subscale 3 score (consequences for personal life) in not family members (n = 7) but the paid caregivers (n = 5: P = 0.01: Table 6).
Discussion
Efficacy of enteral nutrition is considered as great concerns due to its increased use for stroke patients. Several studies examined the risks and benefits of enteral nutrition for long term. For example, enteral formulas containing low amount of selenium and copper have reported to cause selenium deficiency and hematological disorders, respectively [26,27]. However, other studies demonstrated the nutritional benefit and safety of enteral nutrition for long term in cancer, pancreatitis, cystic fibrosis, Crohn's disease, and chronic or end stage of renal failure [28-32]. In a case of stroke patients, most of efficacy studies for enteral nutrition were shortly performed. In this study, we investigated efficacy of enteral formula N for long term in stroke patients. Total of 19 health and nutritional biomarkers were well maintained during the intervention. Particularly, abnormal hemoglobin and hematocrit levels became to be normal according to the enteral nutrition (Table 3). Thus, the enteral formula N may have a potential to improve anemia. In case of home-made enteral formulas, we can infer their inappropriate formulation, compared to the enteral formula N. However, there is a report that average nutrients composition of various kinds of gruels was appropriate [33]. Therefore, we suspect that insufficient calorie intakes cause malnutrition with the use of home-made enteral formulas, rather than formulation issues. Malnutrition can be caused by low calorie intakes in enteral nutrition via rice gruels (per 1 serving size), which have lower calories, compared to dietary reference intakes for Korean per meal [34].
On the other hand, we found that levels of MDA, an oxidative stress biomarker, were higher in the present chronic stroke patients than those in other normal people (our patients, 0.28 ± 0.04 µM; Templar et al. [25]'s normal people, 0.11 ± 0.03 µM). During the 6 months, MDA levels were gradually increased, and it is consistent with previous studies that oxidative stress increases stroke progression [35].
In case of caregiver burden, the present SCQ results were similar to those of other Korean studies (standardized mean of entire scale, duration of stroke; our study, 2.2, 6.0 yrs; others, 2.3, 3.4 yrs) [36]. However, the average of entire scale score in a Dutch study [13] is lower than that of Koreans (Dutch, 47.3; Korean, 59.9). This difference may come from lower mRS scores in the Dutch study than those in our Korean study (mRS of Dutch's, approximately 3.0; Koreans', 4.8). Thus, severe disability of patients may increase caregiver-burden. In another study of dementia patients, Korean and Korean-American caregivers had higher levels of burden, depression, and anxiety than whites, because of social difference, therefore, not only mRS score but also social difference may causes the caregiver-burden variance [37]. In addition, entire scale and subscale 2 (satisfaction with one's own performance as a caregiver) were clearly reduced by the N treatment (Table 4). Considering characteristics of 'subscale 2', we suspect that the enteral formula N induces improvement of caregiver-burden from the satisfaction, which they provide adequately to their patients. As most of commercial enteral formulas have been used with recommendation of hospital experts, e.g. doctors, nurses and nutritionists, during patients' hospitalization (from our unpublished data), the hospital experts' recommendation for formulas is considered to be effective for the caregivers' decision or satisfaction of the formulas.
In the short term study, we examined whether two commercial enteral formulas have equal nutritional efficacy, even they are different in formulations and prices: Price of N is approximately 2 folds lower than J. The results of the short term study showed that both of commercial enteral formulas were somewhat useful to maintain health and nutritional state of acute stroke patients, even though any biomarker level didn't show a significant change during the administration. Most of biomarkers didn't show any difference between the 2 enteral formulas (Table 5). Moreover, improvement of hemoglobin level was better in the N-treatment than that in the J-treatment (Fig. 1). In comparison of formulations, the enteral formula N has 3 fold higher amount of taurine than the enteral formula J (Table 1). Sirdah et al. [38] proved that addition of oral taurine (1,000 mg/day) enhances the RBC, hemoglobin, and ferritin levels in oral iron treated iron-deficiency anemia group due to its antioxidant effects. Therefore, we speculate that high amount of taurine may be related to improvement of the hemoglobin levels (Fig. 1).
Concerning MDA changes, the short term study showed decrease in MDA levels during the intervention, while the long term trial did not. As acute stroke patients can be transiently recovered, compared to chronic patients, the changed MDA levels in the short term trial may come from interaction between characteristics of acute stroke and administration of enteral nutrition N.
In case of life quality, we found that there were no differences in caregiver-burden between N-treated and J-treated groups. In addition, there was heavier burden in subscale 3, i.e. consequences for personal life, among the paid caregivers than family caregivers (Table 6). The paid caregivers' quality of life can directly influence care of the patients. In addition, social need for the paid caregivers is getting more increased. Thus, urgent and various ways, e.g. caregivers' well being, should be prepared to reduce burden of job stress particularly for the paid caregivers.
In conclusion, our study showed that long term usage of commercial enteral nutrition, N, is somewhat effective to maintain nutritional state, particularly anemia-related biomarkers, in dysphagic stroke patients. In addition, the enteral formula N reduces the burden of caregivers with satisfaction of their care activity. Moreover, we evaluate that eneteral formula N has equal nutritional efficacy compared to the formula J, despite of their different prices in the short term trial.



 XML Download
XML Download