

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Pregnant women have been exposed to depression during pregnancy not only because of physical changes due to pregnancy but also because of changes of roles, emotion, and psycho-social characteristics [1]. Kwon [2] supported the stress-vulnerability model of high-risk pregnant women for depression. It has been suggested that risk factors associated with depression during pregnancy include socioeconomic level, occupation, and age of pregnant women [2], and it also has been reported that the mental stress and depression during pregnancy affect the delivery of low birth weight [1] or postpartum delivery [3]. In the study of Kim and Lee [4], factors inducing stress during pregnancy included anxiety for baby, anxiety for health, economic difficulties, depressive feeling, and family relations, and less stress was observed in case of having occupation and more stress in case of larger family size. In addition, higher intakes of energy, fat, phosphorus, potassium, and cholesterol increased the risk for the incidence of pregnancy stress while the intakes of proteins, carbohydrates, dietary fiber, and vitamin B2 decreased the risk for stress. Higher pregnancy stress was observed in pregnant women with higher educational level, and higher stress for physical symptoms of pregnant women and for fatal health were observed in pregnant women with occupation [5]. Park and Lee [6] reported that pregnant women under lots of stress have higher risk for gestational hypertension and pernicious vomiting of pregnancy, and higher stress negatively affected maternal weight gain.
Bodnar et al. [7] observed the positive correlation between BMI and depression during pregnancy, and reported that this affected gestational weight gain. Also, pre-pregnancy overweight has been reported to have a strong correlation with the possibility for depression. In a study of women with the experience of abortion, the subjects underwent very stressful daily life during 3 months before abortion and experienced social difficulties [8], and negatively stressful life events were reported as being related to spontaneous abortion [9]. Also, the administration of ω-3 fatty acid to pregnant women with depression, aged 18~40 years, at 16~32 weeks of pregnancy decreased BDI (Beck Depression Inventory), HAM-D (Hamilton Rating Scale for Depression), and EPDS (Edinburgh Postnatal Depression Scale) [10]. On the other hand, several studies on the relationship among daily life stress, risk of preterm delivery, and short gestational period during 16~30 weeks of pregnancy showed that there is no consistent results on the effect of psychosocial stress on preterm delivery and gestational period [11]. Although the risk of stress and depression during pregnancy has been suggested, there are not enough studies done yet on depression and dietary intakes in pregnant women in the country. Therefore, this study was performed to compare socio-cultural factors, nutrient intake, and pregnancy outcome of pregnant women, according to degree of depression and to prevent depression during pregnancy and to utilize the results as basic data for maternal infant nutrition research.
Subjects and Methods
Subjects and study period
This study was performed through face to face interview in 114 subjects, who agreed for the survey after being explained about this study and who were not twin pregnancy, among pregnant women (first trimester·second trimester·third trimester) who visited the clinic for prenatal care, from February to June of 2009 at an ob/gyn clinic located in Seoul (CHA Hospital IRB 09-03).
Data collection
General characteristics and life style variables
Age, pre-pregnancy BMI, number of pregnancy, education levels, occupation, and the practice of exercise during pregnancy & pre-pregnancy alcohol drinking or smoking were examined from the survey instrument that we developed.
Survey for depression
For the degree of depression in pregnant women, BDI (Beck Depression Inventory), a self-diagnosed depression survey instrument, was used with slight modifications [10], and each of 21 questions was scored on a scale value of 0 to 3. The group with less than 10 points, which was the average score of depression in pregnant women in this study, was classified as low-depression score group, and the group with more than 10 points was as high-depression score group.
Nutrient intake
Dietary intake survey in pregnant women was performed through direct interview using a 24-hour recall method for collecting information on the previous day's dietary intake. During the interview, pictures of food model and food model were used for the accurate dietary intake. Nutrient intakes were analyzed using a nutrition evaluation program, Can-pro (computer aided nutritional analysis program for professionals 3.0).
Iron nutrition indices
Iron indices of pregnant women were examined by using clinical records of the hospital and included WBC (White Blood Cell), RBC (Red Blood Cell), HGB (Hemoglobin), HCT (Hematocrit), MCV (Mean Corpuscular Volume), MCH (Mean Corpuscular Hemoglobin), MCHC (Mean Corpuscular Hemoglobin Concentration), RCDW (Red Cell Distribution Width), PLT (Platelet), PDW (Platelet Distribution Width), and MPV (Mean Platelet Volume).
Statistical analysis
All statistical analyses were performed using SAS software program version 9.1 (SAS Institute, Cary, NC, USA). All measurements were presented as mean ± standard deviation and percentage. Differences in general characteristics, socio-cultural factors, life style variables, nutrient intakes, and iron nutrition indices based on the depression score in pregnant women were verified by using t-test and chi-square analysis. Generalized linear model was used to verify the significance of differences in each survey item and the average birth weight, and each survey item was categorized to suggest the influence of the survey item on major pregnancy outcomes and then multivariate logistic regression was performed with major pregnancy outcome as dependent variable. All statistical tests were two-tailed tests performed at the significant level of P < 0.05.
Results
General characteristics
General characteristics and environmental factors of the subjects are shown in Table 1. The average age of pregnant women was 33.65 ± 3.66 years in LS (low-depression score) group and 33.84 ± 3.22 years in HS (high-depression score) group, which was similar in both groups. For the number of pregnancy, primipara was 54.8% in LS group which was higher than 36% in HS group (P < 0.05), and multipara was 45.2% in LS group which was lower than 64% in HS group, showing significant differences between two groups (P < 0.05). In the educational level of pregnant women, subjects with graduate degrees were 25.8% in LS group and 16% in HS group. The average monthly household income tended to be higher in HS group compared to LS group. Pregnant women with occupations were 52% in HS group which was higher than 46.8% in LS group but not significantly different. The tendency of morning sickness was similar in both groups, and the use of supplementation by pregnant women was also similar in both groups showing 88.7% in LS group and 90% in HS group.
Lifestyle variables
Lifestyle variables of the subjects are shown in Table 2. Pre-pregnancy alcohol drinking experience of pregnant women was 58.1% in LS group and 70% in HS group, showing higher rate in HS group but not significantly. In the drinking frequency during 1 year before pregnancy, less than once a month was 21% in LS group and 38% in HS group, and 1~2 times/week was 4.8% in LS group and 16% in HS group, showing higher drinking frequency in HS group (P < 0.05). Pre-pregnancy smoking experience was 14% in HS group and 8.1% in LS group. The pre-pregnancy smoking period over 7 years was 10% in HS group and 3.2% in LS group. The present coffee intake in pregnant women was similar in both groups but the frequency of coffee intake such as "drink almost everyday" was 30% in HS group and 8.1% in LS group, showing significantly higher intake in HS group (P < 0.01).
Nutrient intakes
Nutrient intakes of the subjects in this study are shown Table 3. Energy intake was 1,888 ± 590.05 kcal in LS group and 1,743.7 ± 937.76 kcal in HS group, and protein intake was 80.5 ± 53.87 g and 67.97 ± 44.82 g, respectively. Also, fat intake was 57.9 ± 31.58 g and 51.99 ± 38.7 g, and carbohydrate intake was 273.12 ± 71.62 g and 254.38 ± 115.45 g, and dietary fiber was 21.63 ± 9.48 g and 18.25 ± 14.14 g, respectively, showing that almost all nutrient intakes tended to be higher in LS group than in HS group. Total calcium intake was 648.33 ± 252.11 mg in LS group and 533.08 ± 251.52 mg in HS group, which was significantly higher in LS group (P < 0.05), and plant calcium was 308.5 ± 118.78 mg in LS group and 252.8 ± 117.39 mg in HS group, which was also significantly higher in LS group (P < 0.05). Plant iron intake was 11.43 ± 8.56 mg in LS group and 8.33 ± 3.02 mg in HS group, showing higher intake in LS group compared to HS group (P < 0.01). Potassium intake was 3,073.1 ± 1192.3 mg in LS group and 2,430.3 ± 881.11 mg in HS group, showing that the intake in LS group was significantly higher (P < 0.001). Total folate intake was 281.15 ± 113.99 µg in LS group and 230.47 ± 89.16 µg in HS group, showing significantly higher intake in LS group (P < 0.05). Also, dietary folate intake was 288.07 ± 128.93 µg in LS group and 229.26 ± 91.94 µg in HS group, showing significantly higher intake in LS group (P < 0.01). In most nutrient intakes, LS group showed higher intake tendency than HS group. The P/M/S ratio was 1/1.4/1.4 in LS group and 1/1.3/1.2 in HS group, showing rather higher tendency of saturated fat intake in both groups compared to the desirable P/M/S ratio of 1/1~1.5/1.
Iron nutrition indices
Iron nutrition indices of the subjects are shown in Table 4. WBC (White Blood Cell) was 9.5 ± 3.01 103/µl in LS group and 9.25 ± 3 103/µl in HS group, which were in the normal range but slightly higher. RBC (Red Blood Cell) was 3.74 ± 0.77 106/µl in LS group and 3.72 ± 0.44 106/µl in HS group, showing similar values in both groups but lower levels than normal range of female adults. HGB (Hemoglobin) and HCT (Hematocrit) was 11.75 ± 1.27 g/dl and 11.34 ± 1.24 g/dl, respectively, and 34.87 ± 3.5% and 33.63 ± 3.76%, respectively, showing similar tendency in both groups but lower levels than normal female adults.
Pregnancy outcomes
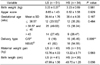
Pregnancy outcome for pregnant women and infants is shown in Table 5. The average birth weight and length were 3.23 ± 0.27 kg and 47.99 ± 1.56 cm in LS group and 3.23 ± 0.69 kg and 48.7 ± 1.26 cm in HS group. Apgar score was 8.65 ± 1.43 in LS group and 8.62 ± 1.58 in HS group, showing no significant differences in average birth weight, length, and apgar score. Gestational period was 39.44 ± 1.76 weeks in LS group and 38.4 ± 4.06 weeks in HS group, showing that 35% of HS group had less than 38.6 weeks of gestational period. Natural spontaneous vaginal delivery was 82% in LS group but 54.6% in HS group, which was significantly different (P < 0.05). Total maternal weight gain during pregnancy was 13.76 ± 4.03 kg in LS group and 13.22 ± 3.71 kg in HS group, showing higher increase in LS group but without significant difference.
Birth weight according to levels of various factors
Birth weight according to levels of various factors is shown in Table 6. As alcohol intake frequency and coffee intake frequency showed difference by depression score when comparing the lifestyle by depression score (Table 2), this was also included in the analysis because of its possible influence on birth weight, but only gestational period showed significant relationship with birth weight. The average birth weight was 2.97 ± 0.1 kg in less than 38.6 weeks of gestational period, 3.31 ± 0.08 kg in 38.6~40 weeks of gestational period, and 3.44 ± 0.1 kg in more than 40 weeks of gestational period, showing significant increase of birth weight as gestational period increased (P < 0.01). For pre-pregnancy BMI, the birth weight tended to increase as BMI increased, and each group showed similar results in depression score, alcohol intake, and coffee intake.
Factors predictable for delivery type
Since delivery type was significantly different by depression score in the univariate analysis, we examined the effect of depression score on delivery type using multivariate logistic regression analysis. The analysis model included birth weight, maternal age, parity and income as covariates. Adjusting for birth weight, maternal age, parity and income, the group with less than 10 points of depression score had significantly lower odds of c/s risk than the group with more than 10 points of depression score (Odds ratio: 0.22, 95% CI; 0.07~0.7) (Table 7).
Discussion
This study was performed to investigate the differences in the lifestyle, nutrient intakes, iron nutrition indices, and pregnancy outcome in pregnant women depending on the depression score. Depression score was significantly different by the number of pregnancy (P < 0.05), showing lower depression score in primipara and higher score in multipara. Hong and Kim [5] reported that pregnant women with occupation had higher stress for physical symptoms of pregnant women and for fetal health, which is rather different from the results in this study.
The lifestyles of pregnant women were not significantly different, but LS group tended to have more women practicing exercise than HS group. The frequency of exercise was also higher in LS group than in HS group. This is similar to the results of Kim and Lee [4] in which the group with less stress during pregnancy practiced light activities and regular exercise than the group with higher stress. Also, a study of pregnant women in Daegu area [12] reported that primipara group exercised more regularly than multipara group, suggesting that primipara group exercises regularly with less stress during pregnancy. Bovbjerg et al. [13] reported that exercise during pregnancy reduced the risk for Cesarean section. It is thought that proper exercise can relieve the stress in pregnant women and lead to desirable pregnancy outcomes. Pre-pregnancy alcohol intake was higher in HS group with higher frequency too (P < 0.05). Sayal [14] in England reported that more than 4 glasses/day alcohol intake in pregnant women increased the risk for fetal behavior and mental health, and that daily drinking before pregnancy increased the risk for hyperactivity and attention deficit. Also, Yang et al. [15] observed that alcohol intake during pregnancy strongly affected abruption placenta (premature separation of placenta). There were no pregnant women who drank alcohol during pregnancy among the subjects in this study but pre-pregnancy drinking frequency was higher in HS group, and thus it is necessary to provide nutrition education and promotion for the lifestyle of not drinking alcohol during pregnancy.
In case of coffee intake frequency, the pre-pregnancy coffee intake ratio was significantly higher in HS group (P < 0.01). In the study on the risk for neural tube damage in pregnant women and their infants with caffeine intake [16], the risk for spina bifida in infants was increased in the group of pregnant women who had more than 10 mg/day caffeine through coffee, tea, soda beverages or chocolate before pregnancy. Thus it is noticeable that pre-pregnancy lifestyle of pregnant women can influence the emotional state of pregnant women and lead to undesirable pregnancy outcomes.
The average daily energy intake of the subjects in this study was 1840.81 ± 774.5 kcal, which is 97~80% of 1,900~2,350 kcal, the EER for pregnant woman in KDRIs (Dietary Reference Intakes for Koreans) [17]. Protein intake was 149% KDRIs (EAR) in LS group and 125% KDRIs in HS group, and most nutrients except vitamin A and sodium tended to have higher intake in LS group compared to HS group. This is similar to the results that energy and protein intakes were higher in low-stress group than in high-stress group [18]. Kim and Lee [4] reported that nutrient intakes were similar in both low-stress group and high-stress group. Total calcium, plant calcium, plant iron, potassium, total folate and dietary folate intakes were significantly higher in LS group than in HS group, respectively (P < 0.05, P < 0.05, P < 0.01, P < 0.001, P < 0.05, P < 0.01), but total calcium & total folate intakes of both groups were under the EAR of the KDRIs. Choi et al. [19] studied the relationship between stress by trimester and nutrient intakes and reported that potassium and vegetable calcium intakes in the early pregnancy were decreased as stress became higher, which is similar to our results. Also, birth weight of infants from pregnant women with stress was lower than that without stress, and apgar score was also lower in the group with stress than that without stress. Czeizel et al. [20] reported that the administration of 0.8 mg/day folate starting from one month before pregnancy reduced the risk for congenital cardiac anomalies and neural tube defects in infants. Also in the study on the intakes of vegetables, fruits, and vegetable oils in pregnant women and the risk for toxemia [21], the higher intake of vegetables reduced the risk for toxemia.
The analysis for iron nutrition indices in pregnant women showed that all values except RBC, HGB, and HCT were in the normal range and no significant differences were observed between LS group and HS group. HGB was 11.75 ± 1.27 g/dl in LS group and 11.34 ± 1.24 g/dl in HS group, and HCT was 34.87 ± 3.5% in LS group and 33.63 ± 3.76% in HS group. These are lower than the normal ranges of HGB and HCT in female adults, 11.5~16.9 g/dl and 36~46%, respectively, but not the level of anemia by WHO criteria, HGB < 11.0 g/dl and HCT < 33.0%, for anemia in pregnant women [22].
For pregnancy outcome, no significant differences in birth weight, birth length, apgar score, total maternal weight gain, and gestational period were observed between two groups. In case of delivery type, the ratio for Cesarean section was significantly higher in HS group compared to LS group (P < 0.01). Liston et al. [23] observed that Cesarean section, when compared to normal spontaneous vaginal delivery, increased the hypo-function and risk for respiratory condition at birth and thus increased the risk for respiratory distress syndrome and transient tachpnoea of the newborn. That is, the possibility for Cesarean section can be increased in pregnant women with higher depression score and affect negatively on pregnancy outcomes. In this study, the gestational period was analyzed as a significantly influential factor on birth weight (P < 0.01).
In the study on the birth weight changes of normal birth in the past 5 years in Korea [24], the average birth weight per gestational period was decreased in the order of 37 weeks, 38 weeks, and 39 weeks and the decrement became smaller as the gestational age increased, suggesting that the maintenance of normal gestational period is important for desirable pregnancy outcomes.
Hedegaard et al. [11] in Denmark reported that the living environment that induced higher stress increased the risk for short gestational period and preterm delivery. Bae [25] also reported lower birth weight from shorter gestational periods, and Maconochie et al. [26] reported that the stress was one of the causes of miscarriage and could be reduced by taking vitamin supplements and eating fresh fruits and vegetables everyday. Thus it is considered that proper lifestyle management including nutritional management is needed for pregnant women because the living environment of a pregnant woman can affect negatively on pregnancy outcome in relation to stress.
The analysis of factors for affecting delivery type in this study showed that only depression score had significant differences (P < 0.01). Olusanya and Solanke [27] reported that delivery type was related to age, occupation, social status, number of pregnancy, and income level, and emergency Cesarean section had apgar score at 5 minutes of less than 7 points and special protective care was needed for infants. Thus it is suggested that the risk for Cesarean section became lower as the depression score decreased (Odds ratio: 0.22, 95% CI; 0.07~0.7).
In this study, LS group tended to have higher exercise frequency compared to HS group, and proper exercise during pregnancy decreased the risk for Cesarean section. In addition, LS group showed lower alcohol and coffee intakes compared to HS group, suggesting the relationship between the lifestyle of pregnant women and desirable pregnancy outcomes. Like this, HS group showed fewer exercise frequency during pregnancy and higher intakes of alcohol and coffee before pregnancy compared to LS group. That is, higher depression score was related to undesirable lifestyle and highly related to negative pregnancy outcomes such as Cesarean section.
Therefore, it is thought that the degree of depression during pregnancy can have important influence on pregnancy outcome. By considering the recent reality of higher childbearing age and lower birth rate faced by our society, it is more important than anything to educate pregnant women and promote proper lifestyle during pregnancy to induce desirable pregnancy outcome, in the aspect of ensuring better human resources.






 XML Download
XML Download