

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
The global prevalence of childhood obesity has risen dramatically and is considered a significant public health problem. Since the 1970s, the prevalence of obesity has more than tripled for children aged 6-11 years in the United States [1]. In Korea, the incidence of obesity among children aged 10-18 years increased from 5.4% in 1998 to 11.3% in 2001, as observed in the Korean National Health and Nutrition Examination [2].
It is necessary to decrease the rate of childhood obesity because obese children and adolescents have various adverse health outcomes not otherwise typical for their age, including hypertension, dyslipidemia, and metabolic syndromes [2-4]. Moreover, obese children and adolescents are more likely to become obese as adults and are at higher risk of cardiovascular related diseases, such as high blood pressure, high cholesterol, and type 2 diabetes, than are other children and adolescents [5,6].
The importance of healthy eating habits and regular physical activity has been emphasized to prevent and reduce the rate of childhood obesity because obesity results from an imbalance between energy intake and energy expenditure. Overconsumption of energy because of an increased availability of high calorie and high fat fast foods and larger portion sizes contributes to increased obesity rates [7,8]. Studies have shown that people eat more when presented with larger packages or portions of food [9,10]. Moreover, when eating from larger packages, people underestimate their own consumption to a larger extent compared with when they eat from smaller packages [11]. In addition to increased energy intake, sedentary lifestyles in adolescents play a role in increased prevalence of obesity. In particular, watching television and playing computer games are associated with unhealthful snacking patterns, including low fruit and vegetable intake and overconsumption of energy and fat [12].
Although healthy eating habits and daily physical activity are recommended to prevent childhood obesity, there is no research focused on nutritional status associated with physical activity levels in elementary school students. A better understanding of the relationship between nutritional status and physical activity can help promote education to improve health outcomes. Therefore, the purpose of this study was to determine dietary intake of Korean elementary school students and to examine nutritional status by physical activity level in Korean elementary school students.
Subjects and Methods
Subjects
This cross-sectional study recruited 324 children from grades 4 through 6 (159 boys and 165 girls, age 10-12 years), in an elementary school in Seoul, Korea. A total of 287 students (143 boys and 144 girls) completed the study. A total of 37 students were excluded due to incomplete responses (n = 12) and no information of height and weight (n = 25). The study was conducted from September 2008 to October 2008. Informed consent was obtained from all subjects before start of the study. This study followed Good Clinical Practice (GCP) guidelines.
Anthropometric measurements
Weight and height were measured and body mass index (BMI) was calculated as weight (kg)/ height2 (m2). BMI-for-age was plotted on sex-specific Korean national growth charts. Obese was defined as BMI-for-age ≥ 95th percentile, overweight was defined as values between the 85th and 95th percentiles, and underweight was defined as values < 5th percentile [13].
Physical activity measurement
Physical activity was assessed by using a modified Godin leisure-time exercise questionnaire [14]. A total physical activity score was calculated by summing the frequency (times per week), duration (minutes per session), and intensity of exercise each student performed. Information on the number of months for which the student had been participating in the physical activity was also included in the total physical activity score. An exercise frequency of 1-2 times per week was coded as 1.5, 3-4 times per week was coded as 3.5, 5-6 times per week was coded as 5.5, and daily exercise was coded as 7. Physical activity durations of 10 minutes were coded as 0.17, 15-20 minutes were coded as 0.29, 30-60 minutes were coded as 0.75, and longer than 60 minutes were coded as 1. Physical activity participation for one month was coded as 1, 3 months was coded as 2, 6 months was coded as 3, and 12 months was coded as 4. After the subjects were divided by gender, they were assigned into three groups within the same gender based on the total physical activity scores; children with the highest tertile of total physical activity scores were categorized as active and children with the second highest tertile as moderately active. The others, who had the lowest tertile of total physical activity scores, were categorized as sedentary.
Dietary intake assessment
Dietary intake was assessed with a 24-hour food recall method, which has been proven in a previous study to effectively assess the dietary intake of children as young as 8 years old [15]. Two-dimensional portion size models were provided to enhance the reporting accuracy of the amount of food consumed. Data from the 24-hour recall were analyzed using CAN Pro 3.0 software, developed by the Korean Society of Nutrition (Seoul, Korea) and containing the nutritional values of Korean foods. Nutrient intakes were compared with recent Korean dietary reference values [16].
Statistical analysis
All analyses were performed with SPSS version 12.0 software (SPSS Inc., Chicago, IL, USA). A sample size calculation using data from a previous study [17] was conducted; this analysis indicated that 287 subjects would be required to detect a difference in daily energy intake with 85% power and α = 0.05. Data were presented as mean ± standard deviation (SD). Descriptive statistics were used to report subjects' average age, BMI, and BMI category. Due to the small number of subjects who were not at normal BMI category, nutrient intake data were age-, BMI-adjusted. Analysis of variance (ANOVA) was conducted to test for global significant differences of nutrient intakes by physical activity levels. If the global ANOVA results were significant, a post-hoc analysis with Duncan's multiple range test was used for pair wise comparisons. Results were considered statistically significant only if the P-value of an analysis was < 0.05.
Results
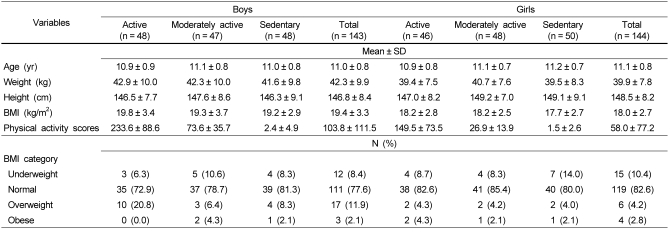
Subjects' age and anthropometric data by physical activity level are shown in Table 1. Subjects (n = 287) were between the ages of 10 and 12 years, with a mean age of 11.1 years and mean BMI of 18.7 kg/m2. Most children (77.6% of boys, 82.6% of girls) were normal weight and 14.0% of boys and 7.0% of girls were either overweight or obese. In addition, mean physical activity score in active boys was 233.6 while it was 149.5 in active girls.
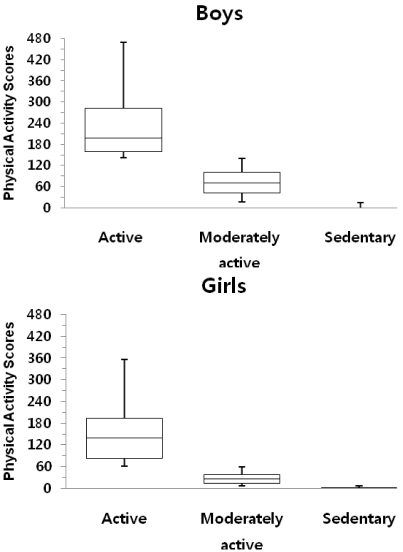
Distribution of physical activity scores among boys and girls is provided in Fig. 1. The median physical activity scores was 198 in active boys and it was 70 in moderately active boys. Girls had lower median physical activity scores than boys, so the median physical activity score in active girls was 140 and it went down to 26.25 in moderately active girls.
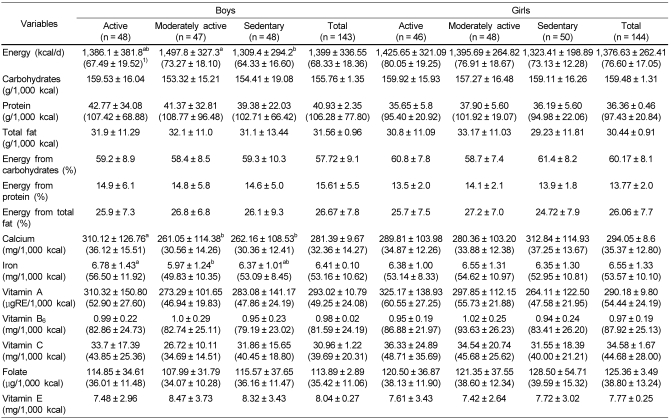
Dietary intakes of the children by level of physical activity are presented in Table 2. The dietary intake analysis showed that daily intake of total energy was higher in moderately active boys than in sedentary boys (P = 0.0074). Total energy intake and energy intake from fat (%) were within recommended ranges among boys whereas protein intake per 1,000 calories was above the recommended intake.
The higher total energy intake of moderately active boys than sedentary boys may have contributed to higher absolute intake of nutrients (P < 0.05), so nutrient density of each nutrient was calculated. Intakes of iron per 1000 calories in moderately active boys were significantly lower than in active boys (P = 0.033 and P = 0.015, respectively). Vitamin C intake also showed the similar trend with iron intake although it was not significantly different among groups.
In contrast to boys, calcium, iron, and vitamin C intakes among girls were not different depending on the level of physical activity. However, intakes of total energy and vitamin A per 1,000 calories tended to be higher in active girls as compared with sedentary girls although they were not significantly different. Both protein and vitamin B6 intakes per 1,000 calories tended to be higher in moderately active girls than in active girls. Total energy intake and energy from total fat (%) among girls were within recommended ranges, but protein intake was above the recommended intake.
For both boys and girls, all micronutrient intakes were lower than Korean reference values. Iron intakes were 53% and 54% of recommended intakes for boys and girls, respectively. Vitamin A intakes were also only 49% and 54% recommended intakes for boys and girls, respectively. Intakes of calcium, vitamin C, and folate for boys and those of calcium and folate for girls were below 40% of recommended intake.
Discussion
The study results suggest that moderately active boys had higher energy intakes than sedentary boys (P < 0.05), but it was not applied to girls. Interestingly, moderately active boys had lower calcium and iron intakes than active boys despite higher energy intake.
In the current study, nutrient intakes of participants were lower than the results from a limited body of research among this age group of Korean showing that children aged 11 years ate approximately 1,700 kcal/day [18,19]. However, acceptable macronutrient distribution ranges of our participants were within recommended with 57.7% from carbohydrate, 15.6% from protein, and 26.7% from fat for boys and 60.2% from carbohydrate, 13.8% from protein, and 26.1% from fat for girls. American children at this age group consumed on average 1766 kcal/day and 33% of calories from fat [20], which are higher than the results of our estimate of intakes.
Both boys and girls had much lower intakes of all nutrients than Korean dietary reference intakes recommended by the Korean Society of Nutrition except for protein intake, which must be due to a lower total energy intake. Regardless of physical activity level, intakes of calcium, vitamins A and C, iron, and folate were lower than recommended values for both boys and girls. In particular, intakes of calcium, vitamin C, and folate for both boys and girls were less than 50% of the recommendation, reflecting low intakes of vegetables, fruits, and milk and milk products. For this age group, low intakes of iron and calcium need special attention. Iron requirements are increased dramatically in adolescents due to the expansion of blood volume, increases in muscle mass, and menarche. The low iron stores caused by insufficient dietary intake of iron in the female adolescents make them susceptible to iron deficiency anemia [21]. In addition to iron intake itself, intake of an enhancing agent(s) of iron absorption, such as vitamin C, must be taken into consideration. Vitamin C enhances intestinal absorption of iron by reducing iron from ferric to ferrous iron [22]. Hence, the current low dietary intakes of iron and vitamin C could cause the students to be at high risk of developing iron deficiency anemia.
Moreover, calcium is another important nutrient for adolescents; sufficient intake of calcium in youth is crucial for achieving optimal peak bone mass [21]. Failure to achieve peak bone mass increases the risk of osteoporosis later [23]. Nutrition education focusing on a balanced diet is necessary to provide proper nutrients for pre-adolescents' growth and development.
Higher tendency of intake of protein in moderately active girls may be related to higher tendency of intake of vitamin B6 in the group because foods high in protein also contain high amounts of vitamin B6 [22].
It is surprising that both boys and girls in the sedentary group did not have higher energy intakes than others because physical inactivity, such as television watching and video or computer games is associated with high energy and fat intakes [12]. The observation that boys were more active than girls is consistent with other study results [20,23,24-26] and different physical activity interventions should be conducted to girls to encourage high rates of participation.
Since little research has been conducted to investigate the association between physical activity level and dietary intake in elementary school students, it is challenging to compare our results with those of previous studies. This is further complicated by differences in environment and subject characteristics, including age and ethnicity. Nevertheless, physical activity level was not related to nutrient intake of Korean middle school students [27]. In contrast, lower energy intake was observed in active Korean adult females as compared to their sedentary Korean adult females. Korean males have reported that an active group consumed higher intakes of calories and fat, within the recommended ranges, than a sedentary group [17,28,29]. Interestingly, Korean males in the active group were already either overweight or obese, which might have caused them to be health conscious and more likely to work out regularly in order to lose weight [28,29].
The positive relationship between physical activity and dietary intakes among adults has been reported to previous studies conducted in Western countries. Beitz [30] reported higher intakes of vitamins B1, B12, E, calcium, and magnesium in active German males than in sedentary German males. Other research has also shown higher intakes of calcium, folate, and vitamins A, C, and E in active adults than in sedentary individuals [31,32]. Furthermore, a population-based study reported that physical activity was inversely correlated with dietary fat intake in American adults from the 1990 Behavioral Risk Factor Surveillance System [33]. Similarly, Eaton et al. [34] reported that moderately active and very active individuals consumed more fiber, vitamins A, C, and E and calcium but less total fat and saturated fat.
Unlike previous studies, the present study did not show an association between dietary intake and BMI possibly due to small number of overweight and/or obese subjects. These results indicate that the active boys in the current study have healthy lifestyle patterns reflected by total energy and fat intakes within recommended ranges.
In this cross-sectional study, elementary school students did not meet their nutritional requirements, except protein for boys. Eating habits are generally formed during early childhood [35] and unhealthy dietary habits appear to grow during the years between elementary and high school [36]. Along with increased bad eating patterns, physical activity declines throughout adolescence [37]. Therefore, the combined insufficient nutrient intakes and physical inactivity in our sedentary subjects may results in poor and slow development and growth and increased risk of chronic diseases, such as obesity, diabetes, and heart disease. The importance of initiation of the healthy eating and physical activity intervention should be emphasized in preadolescence and the intervention should be implemented.
One limitation of this study is the possibility of measurement error. Self-reported measures of dietary intake and physical activity may not be always accurate reflections of these factors. Another limitation is that most subjects were within the normal BMI category, which limits the application of the results to overweight and obese children.
In summary, most Korean elementary school students were either moderately active or sedentary. Nutrient density was not significantly different based on physical activity level, but overall nutritional status was not adequate. Therefore, providing proper nutrients and calories for growth and development in this age group is critical. Targeting interventions to improve both dietary intake and physical activity may cause synergistic health benefits. Because habits developed during early childhood will be maintained in adulthood, proper education regarding a balanced diet and optimum physical activity is required for children's health and growth.
 XML Download
XML Download