

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
The prevalence of vitamin B12 deficiency was underestimated in the past for several reasons, including the erroneous belief that deficiency is unlikely except in strict vegetarians or patients with pernicious anemia, and that it usually takes ~20 y for stores of the vitamin to become depleted [1].
Numerous reports have indicated the increasing prevalence of low vitamin B12 levels among different segments of the general population [2-5]. Poor vitamin B12 status is associated with neurological problems [6,7], hematological disorders [6,8], and other health-related conditions, including poor cognition and Alzheimer's disease [9,10], depression [11], hearing loss [12], cancer [13], and poor bone health [14,15]. Recently, the rapid aging of many populations has increased attention to vitamin B12.
It is known that more vegetarians or elderly people suffer from vitamin B12 deficiency compared to omnivores or younger adults. Because natural sources of vitamin B12 in human diets have known to be restricted to animal-origin food, it has been believed that those people with low animal food diets are more susceptible to cobalamin deficiency [16]. However, vitamin B12 also exists in soybean-fermented foods, seaweeds, and tea leaves [17-19]. Recently, we reported that doenjang, a Korean soybean-fermented paste, contained 0.04-1.85 µg cobalamin/100 g, and that dried laver contained 66.76 µg/100 g (laver is normally consumed in dried form); these figures are surprisingly high compared to those of 0.9-1.2 µg/100 g for eggs [20], and also 1.33 µg per one sheet of dried laver (2 g) was higher than 0.45-0.6 µg per one egg (50 g) when calculated B12 content per one serving size.
In terms of the relationship between vitamin B12 and aging, it has been reported that atrophic gastritis increases with aging, thereby inducing decreased production of the gastric acid and digestive enzymes that are needed to cleave protein-bound vitamin B12 from the natural chemical form of vitamin B12 found in foods. Therefore, Americans aged over 50 years have been advised to consume vitamin B12 in the crystalline form [6].
Historically, Koreans have consumed a plant-based diet including steamed rice, staple food. Even today, the elderly, especially those living in rural areas, adhere to this traditional diet, even though young people have moved toward Western dietary patterns. There has been concern that vitamin B12 status among the elderly is poor. However, data are not available on vitamin B12 status and intake among elderly Koreans, and only a few reports have been published regarding vitamin B12 intake or serum vitamin B12 level among young adults [21,22] and pregnant women [23]. Moreover, the vitamin B12 intake in extant reports are considered to represent underestimates because the Korean national database on vitamin B12 content in foods does not contain data on plant-origin foods. Recently, we analyzed some plant-origin foods widely consumed in Korea [20], and updated this database accordingly.
In this study, we first assessed the vitamin B12 status and intake pattern among very old elderly female Koreans living in rural areas by measuring serum vitamin B12 level and estimating daily vitamin B12 intake. Especially, we were interested in how much some unique plant-origin foods consumed by Koreans, such as soybean-fermented foods, seaweeds and kimchi, contribute to their vitamin B12 intake.
Subjects and Methods
Subjects
Females aged 85 years and older were recruited in rural areas in Korea during summer of 2003 to 2005. Candidates were randomly selected based on birth records, and those living in facilities were excluded. Our research team including dietician, nurse, medical doctor and students visited each home after getting the consent. We kept the ethical and standard of institutional review board of author's institute and the Helsinki Declaration during this study. For recruiting subjects, we explained about the purpose and process of this study to Government officer and village leaders, and also explained and took the consent from every candidate or her/his family member. Finally, 127 subjects, including 70 centenarians, participated in our study. The age of the subjects ranged from 85 to 108 years, and the average age was 98.0 ± 5.7 years. The age distribution of subjects is shown in Table 1.
Food and nutrient intake including vitamin B12
Well-trained interviewer wrote down one-day diet history of each subject by 24-h recall and weighing method with the help of her/his family members. The intake of dairy product, meat and eggs, fish and shellfish, cereals, potatoes and starch, sweets, legumes and tofu, vegetables and seaweeds, fruits, and soybean-fermented foods, as well as total food intake were calculated. The energy and nutrient intake of subjects were calculated using a computer software package, CAN-Pro 2.0, developed by the Korean Nutrition Society. In particular, we calculated daily vitamin B12 intake and the proportions of vitamin B12 from plant-origin foods such as soybean-fermented foods, seaweeds, kimchi and etc.
Results
Food intake
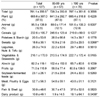
The food intake pattern is shown in Table 2. The average total food intake of subjects was 761.1 g/day. Meals were comprised primarily of plant foods (87.5% of total) such as cereals, legumes and their products, vegetables, fruits, and so on. The average intake of cereals was 232.6 g/day, and almost of this consumption derived from rice, a staple food for Koreans. The subjects consumed 26.3 g/day of legumes, nuts, and tofu, a representative soybean product consumed in Korea. They consumed 216.1 g/day of vegetables and seaweeds, including 82.2 g/day of kimchi, the most popular vegetable-fermented food in Korea, and large portion of vegetable intake was derived from various blanched vegetables (namul in Korean). They also consumed 23.1 g/day of soybean-fermented foods, such as doenjang, chungkookjang, gochujang, and ganjang. The average fruit intake was 71.0 g/day. On the other hand, subjects consumed 95.5 g/day of animal foods (12.5% of total), including 52.7 g of meat, poultry, and eggs; 30.9 g of fish and shellfish; and 10.8 g of dairy products.
On comparing the food intake patterns between the 85-99 yr-old group and centenarians, centenarians consumed significantly more dairy products (P < 0.05) and sweets (P < 0.001) than the 85-99 yr-old group did, because some centenarians enjoyed candy and consumed yogurt. However, no significant differences in the consumption of the other food groups or in the ratio of animal to plant food intake were found.
Energy intake and vitamin B12 Intakes
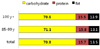
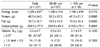
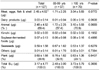
Daily energy and protein, fat, carbohydrate and vitamin B12 intake of subjects are shown in Table 3. The average energy intake was 1,229 ± 457 kcal/day which is 76.8% of the estimated energy requirement (EER) for Korean women aged 75 and over, 1,600 kcal/day [24]. The average energy intakes in the 85-99 yr-old group and centenarians were not significantly different; 1286 ± 510 kcal/day in the 85-99 yr-old group, and 1,186 ± 418 kcal/day in centenarians. The subjects consumed 49.3 g of protein/day, 109.6% of the recommended intake (RI) of protein, 45 g/day [24], even though they consumed less animal foods. As shown in Fig. 1, 70.6% of energy was from carbohydrates (220.5 g/day); 15.5% from protein and 13.9% from fat, and these proportions were not significantly different between the two age groups.
In terms of vitamin B12, our subjects consumed 3.17 ± 4.77 µg/day of vitamin B12, which is about 132% of RI for Korean adults, 2.4 µg/day [24]. There was no significant difference in daily mean vitamin B12 intake between the two age groups (2.48 ± 3.00 µg/day in the 85-99 yr-old group and 3.73 ± 5.79 µg/day in centenarians). In total subjects, 52.7% consumed less than 2.0 µg/day, estimated average requirement (EAR) for vitamin B12 for Korean adults (Table 3).
Dietary source of vitamin B12
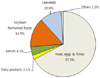
Dietary sources of vitamin B12 are listed in Table 4. The percentages of vitamin B12 intake derived from animal food and plant food were 69.4% and 30.6% of total vitamin B12 intake, respectively. The primary source of vitamin B12 was clearly meat, eggs, and fish, which provided 2.45 ± 4.52 µg/day (67.3% of total intake); the secondary was soybean-fermented foods, providing 0.07 ± 0.13 µg/day (14.5%); the tertiary was seaweeds, providing 0.59 ± 1.58 µg/day (10.8%) (Table 4 & Fig. 2), and kimchi also provided 0.02 ± 0.03 µg/day (4.3%). The average intake of vitamin B12 and the sources did not differ between the two age groups.
Serum vitamin B12 concentration and association with dietary intake
The mean serum vitamin B12 concentration was 450.5 ± 226.9 pg/mL; 477.1 ± 172.7 pg/mL in the 85-99 yr-old group and 441.5 ± 243.1 pg/mL in centenarians without significant difference between the two age groups (Table 5).
It has been widely accepted that adults with serum vitamin B12 level under 200 pg/mL are highly likely to be vitamin B12 deficient [25,26]. By the same criteria, 9.6% (4.8% of the 85-99 yr-old group and 11.3% of centenarians) were assessed to be vitamin B12 deficient. The prevalence of low serum vitamin B12 was not significantly different between the two age groups (Table 5).
It was not observed a significant correlation between serum vitamin B12 concentration and dietary intake (P=0.4769). However, vitamin B12 intake was significantly lower (P < 0.001) in the subjects with low serum vitamin B12 (0.79 ± 0.79 µg/day) than those in normal subjects (3.47 ± 5.72 µg/day) (Table 6).
Discussion
It is well known that the metabolism of vitamin B12, folate, and homocystein are associated in humans and play very important roles in preventing cognitive impairment in the elderly [27-29]. Risk factors for vitamin B12 deficiency include low animal protein intake, malabsorption associated with atrophic gastritis or Helicobacter pylori infection, pancreatic or intestinal pathology, and gastric acid-reducing medications [6,30-32]. Malabsorption of vitamin B12 from food is the main cause of deficiency in the elderly and explains why depletion occurs with aging. The condition is caused by atrophy of gastric mucosa and the gradual loss of gastric acid, which releases the vitamin from food. The low gastric pH that occurs as a result of gastric atrophy can also increase bacterial overgrowth in the upper intestine, which results in less absorption of protein-bound vitamin B12. Approximately, 10-30% of older adults suffer from malabsorption of protein-bound vitamin B12 [6].
Serum vitamin B12 concentrations < 150 pmol/L (200 pg/mL) indicates frank vitamin B12 deficiency, but there is no widely accepted biochemical cutoff for marginal or preclinical vitamin B12 deficiency or vitamin B12 adequacy [6]. The use of both serum vitamin B12 and methylmalonic acid (MMA) or holotranscobalamin is more recommended to improve diagnosis of vitamin B12 deficiency [25,26]. However, it is limitation s to use MMA level for simple screening of the vitamin B12 status because MMA measurement needs mass spectrometry which is not easily available and needs trained labor and high cost.
It has been reported that, depending on the biochemical criteria for vitamin B12 and/or MMA, approximately 5 - 20% of elderly individuals are deficient in vitamin B12 in the Americans [1,6,30,33]. Pfeiffer et al. [34] reported that the prevalence of vitamin B12 deficiency (serum concentration < 200 pg/mL) in US population varied by age group and affected ≤ 3% of those aged 20-39 y, ~4% of those aged 40-59 y and ~6% of persons aged ≥ 70 y, and plasma MMA concentration were markedly higher after > 60 y. The prevalence of vitamin B12 deficiency increased substantially after 69 y in 3 UK surveys; it affected about 1 in 20 people aged 65-74 y and at least 1 in 10 of those aged ≥ 75 y [1].
Originally, we expected that vitamin B12 deficiency would be more prevalent in our subjects than in subjects of Western countries because our cohort were included many centenarians and had been eating a greater proportion of plant foods. However, only 9.6% of our subjects showed low vitamin B12 concentration (< 200 pg/mL), which was lower than those of Western cohorts. So far, there were very few reports on vitamin B12 status or intake in subjects aged 85 and more. The mean serum vitamin B12 concentration of our subjects, 450.5 pg/mL (337 pmol/L), was similar to 332 pmol/L of an elderly cohort (mean age 76.4 years) in the US [30], but lower than 358 pmol/L of 71-74 y-old female Norwegian cohort [35].
The relation between dietary intake and vitamin B12 status has been investigated in different populations, with conflicting results. One study concluded that low vitamin B12 status in the elderly was not related to inadequate intake [36], whereas other reports showed significant associations between intake of vitamin B12 and plasma concentrations [37,38]. Recently, Vogiatzoglou et al. [35] reported that the association of plasma vitamin B12 with food intake was weaker in older subjects than in younger subjects, and that plasma vitamin B12 was associated with intakes of increasing amounts of vitamin B12 from dairy products or fish but not with intakes of vitamin B12 from meat or eggs. In the present study, it was not observed significant correlation between dietary intake and serum vitamin B12 concentration (P=0.4769), however, the dietary intake of the subjects with low serum vitamin B12 (< 200 pg/mL) was significantly lower (P=0.0005) than that of the subjects with normal serum normal serum vitamin B12.
Our subjects consumed dietary vitamin B12 (3.17 µg/day) less than that in female subjects aged 85 and older in Austria (3.9 µg/day) or the UK (4.3 µg/day) [39]. Interestingly, the dietary source of vitamin B12 intake was totally different. Whereas our subjects were taking 30.6% of total vitamin B12 intake from plant-origin foods, mainly soybean-fermented foods, seaweeds and kimchi, female Norwegian aged 71-74 y were taking 5.0 µg/day of vitamin B12, which was entirely from animal foods; 52.7% from meat, fish and eggs and 47.3% from milk and dairy products [35].
Most of Koreans enjoy fermented foods, such as doenjang (soybean-fermented paste), ganjang (soy sauce) and gochujang (Red pepper, soybean & starch-fermented paste), and kimchi (vegetable-fermented foods) every day, and seaweeds very often. Therefore, it is considered that these foods are very helpful in protecting the elderly Koreans from vulnerability to vitamin B12 deficiency. Some edible algae, including laver, have already been reported to contain large amounts of vitamin B12 [20,40]. Takenaka et al. [41] have demonstrated that the vitamin B12 in dried purple laver is bioavailable to mammals.
This study has some limitations. First and foremost, only a one-day diet record was collected. Second, serum data number was small in 85-99 yr-old group. Third, the updated food composition table on vitamin B12 is still not large enough to cover all foods consumed by subjects. Fourth, the references of RI and EAR for nutrients for the elderly people aged 75 years and older were used, because those for very old people aged 85 years and older are not yet established. Nevertheless, this study is of value because it represents the first report on vitamin B12 intake pattern and serum level in a very old elderly Korean cohort, including centenarians, and also because it elucidates the big contribution of Korean traditional foods to the dietary vitamin B12 intake of this population.



 XML Download
XML Download