

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
African Americans are one of the largest ethnic minority groups in the United States (U.S. Census Bureau, 2008). African Americans in the United States suffer from many health disparities related to chronic diseases. For example, the rate of obesity is higher among African Americans compared to white Americans (National Center for Health Statistics, 2008). Also, African Americans have higher rates of obesity-related co-morbidities such as diabetes, hypertension, cerebrovascular disease, and some cancers than the white population (Satia et al., 2004).
North Carolina has the 17th highest rate of obesity in the nation among adults and 5th highest among teens. It is ranked 9th highest for rates of diabetes and 10th highest for hypertension (Trust for America's Health, 2008). In 1999-2002, the rate of death from heart disease among black North Carolinians was more than 20 percent higher than in whites (Center for Disease Control and Prevention, 2008; North Carolina Department of Health and Human Services, 2008). Additionally, while the cancer mortality rate in the nation declined over the last decade, cancer mortality remains high in North Carolina, and in Edgecombe County, NC where blacks comprise the majority of the population, it is the number one cause of death (North Carolina State Center for Health Statistics, 2008).
Lifestyle factors including diet and physical activity play an important role in prevention of these health conditions. Diets that include daily consumption of a variety of fruits and vegetables, whole grains, limited or moderate use of low fat meats and dairy products have been found to assist in the prevention of many chronic diseases (Office of Disease Prevention and Health Promotion U.S. Department of Health and Human Services, 2008). The National Cancer Institute recommends that black men eat 9 servings of fruits and vegetables a day as part of an active lifestyle to promote good health and protect against diet-related diseases (National Cancer Institute, 2008). Additionally, an objective of Healthy People 2010 is to increase the proportion of people consuming at least two servings of fruits and three servings of vegetables. In addition, objectives of Healthy People 2010 include increasing the proportion of people who consume at least three servings of whole grains, and who consume less than 10 percent of total calories from saturated fat. Unfortunately, many Americans do not meet recommendations. According to Healthy People 2010, food consumption patterns of citizens 2 years of age and older in the United States reflect insufficient daily consumption of whole grains (7% meeting recommendations), vegetables (3%), and fruits (28%) (Healthy People 2010, 2008).
The traditional cuisine of African Americans in the southern U.S. is often called "soul food." Although soul foods include a variety of healthful foods such as collards, okra, rice, legumes, and sweet potatoes, soul foods also include high intakes of fat from a variety of meats, especially pork, seasoned with lard or other animal fats. According to a recently published study with African Americans living in North Carolina, fat intake comprised close to 50% of calories which far exceeds the current recommendation of 20 to 35% of calories from total fat (Kim et al., 2008). Also, intake of fruits and vegetables among black North Carolinians is particularly low. Satia et al. (2004) reported that the mean daily intake of fruits and vegetables was 0.88 and 1.64 servings, respectively, among African Americans living in North Carolina.
The objectives of this research project were to 1) assess participants' nutrition knowledge and knowledge of food and disease prevention linkages, 2) assess perceived benefits of and barriers to eating a healthy diet, 3) assess self-efficacy associated with eating a healthy diet, 4) assess beliefs about healthfulness, appropriate consumption, and protective aspect of specific foods including fruits, vegetables, and whole grains, and 5) identify self-efficacy of shopping for foods such as whole grains, foods low in fat or sodium among members of two African American churches located in two eastern North Carolina counties.
Subjects and Methods
Subjects
Surveys were collected from a convenience sample of 57 African Americans who lived in either Pitt or Edgecombe counties of North Carolina. In 2006, African Americans made up approximately 34% of Pitt County's population while most (about 57%) of Edgecombe county residents were African Americans. Surveys were administered at a church setting. Participants were instructed to take the survey home, fill it out and bring it back to the church where completed surveys were collected.
Survey development
The perception of eating a healthy diet was assessed using a survey developed for this research project. The survey included knowledge questions about nutrient content of different foods, dietary recommendations for fruits and vegetables intake and association between diet and disease prevention. The survey also contained questions on decisional balance (benefits and barriers) and self-efficacy statements regarding eating a healthy diet. Additionally, questions about how healthy foods such as fruits, vegetables, whole grains, red and processed meats were believed to be, about beliefs regarding personal adequacy of intake of these foods, and about beliefs regarding which foods may help prevent certain chronic diseases such heart disease, diabetes or hypertension, and about grocery shopping patterns were included in the survey (Table 4).
The development of the survey followed the following five steps:
literature search to select statements that measured benefits, barriers, and self-efficacy,
creation of statements about knowledge, how healthy are foods such as fruits, vegetables, whole grains, red and processed meats, beliefs regarding adequacy of intake of these foods, beliefs about foods that may prevent from certain chronic diseases such as heart disease, diabetes or hypertension, and about grocery shopping patterns of participants,
consultation with an African American Registered Dietitian with an extensive experience in faith-based nutrition intervention program regarding content validity of the survey,
cognitive testing of the survey, and
analysis of internal consistency of statements within decisional balance and self-efficacy.
Decisional balance and self efficacy
The survey included statements related to decisional balance (11 for benefits and 12 for barriers) and 16 self-efficacy statements regarding eating a healthy diet. All of these statements were rated on five-point scale. All the decisional balance statements on the rated scale included options of 1-strongly disagree, 2-disagree, 3-neither agree/disagree, 4-agree, and 5-strongly agree. The Cronbach alpha reliability scores for the decisional balance statements were 0.956 for benefits and 0.904 for barriers.
The self efficacy statements included statements within three subscales: seven statements within negative affective subscale, three statements within positive social subscale and six statements within difficult/inconvenient subscale (Table 2). These subscales were used to assess self efficacy of eating a healthy diet. Additionally, efficacy of shopping for foods low in fat, sodium or purchasing whole grains was included in the survey (Table 2). All of the self-efficacy statements items were rated as 1- not at all confident, 2-not confident, 3-neither, 4-confident and 5-very confident. The Cronbach alpha scores for the self-efficacy subscales were 0.951 for the negative affective scale, 0.611 for the positive social scale, and 0.879 for the difficult/inconvenient scale. The Cronbach alpha score for the self-efficacy to shop for foods such as whole grains, foods low in fat or sodium was 0.936.
Beliefs and knowledge statements
Beliefs about how healthy are foods such as fruits, vegetables, whole grains, red and processed meats were assessed using 11 statement on a five scale including 1-very unhealthy, 2-somewhat unhealthy, 3-neither healthy/unhealthy, 4-somewhat healthy, and 5-very healthy (Table 3). Also, participants could select I do not know option scored as 0. Beliefs about foods/dietary supplements that may prevent from certain chronic diseases such heart disease, diabetes or hypertension included 11 statement scored 1-does not at all prevent, 2-not prevent, 3-neither, 4-prevent, 5-strongly prevent, and 0-I do not know. Beliefs about intake included 11 statements scored 1-I eat some but not enough, 2-my intake is about right, 3-I should eat more of it/them, 4-I should eat less of it/them.
The survey also included question about perception of intake of specific foods including whole grains, fruits, vegetables or meats (Table 4). These questions had four possible answers to choose from including I eat some but not enough, My intake is about right, I should eat more of it/them and I should eat less of it/them.
Twenty statement in the survey assessed participants' nutrition knowledge (Table 6). Eleven of these statements were designed to assess knowledge about nutrient content, two about dietary recommendations and seven about disease prevention. Nutrient content statements were multiple-choice and included questions such as Which of the following foods have the highest content of trans fats? The two multiple-choice statement regarding recommendations asked for current recommendation for intake of fruits and vegetables. A statement Eating adequate amounts of fruits may help prevent cancer is an example of questions about disease prevention. The disease prevention statements included Yes, No, and I don't know answers.
Content validity and cognitive testing
During the process of the survey development the researchers met with an African American dietitian who had an extensive experience in faith-based nutrition interventions to review the content of the survey. As a result, several statements in the survey were modified. For example, one of the statements in the survey asked about the health effects of nuts. The dietitian suggested to include specific examples of nuts such as peanuts, pecans and walnuts. Similarly, examples of processed meats (e.g. sausages, hotdogs) were also given to clarify questions.
Three African American church members were asked to participate in the cognitive testing of the survey to assess the understandability and readability of the instrument. As a result, several statements were rephrased. For example, a statement Please rate each of the following barriers to eating healthy foods was rephrased as Please rate how confident you feel about eating healthy foods under each circumstance. In addition, changes to the demographical information included in the survey were made. For example, in-stead of Gender: Male Female, a phrase I am Male Female, (circle one) was suggested.
Results
Demographic
Fifty-seven African Americans who were on average 50 years old (SD 12.70) completed the survey. The majority of respondents (58.1%) were female and most (75%) had at least some college education. About 96% of participants were either overweight or obese (BMI≥25). About 52% had annual income below $35,000.
Decisional balance and self-efficacy
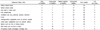
Each of the benefit statements included in the survey was scored higher than any of the barrier statements (Table 1). The lowest mean score for the benefits statement was considerably higher than the highest mean score for the barriers (4.12 vs. 3.68). A statement Eating healthy foods would help me to take care of my body received the highest mean score (4.79) from all benefits statement while "Healthy foods are too expensive" included in the barriers variable had the highest score (3.68). On the other hand a belief that Eating healthy foods would help me to look young included in the benefit subscale received the lowest score (4.12) while I do not know how to find healthy foods in a grocery store was scored lowest among the barrier statements (2.19).
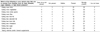
The mean self-efficacy subscale scores were 3.33 for the negative affective subscale, 3.72 for the positive social subscale and 3.21 for the difficult/inconvenient scale. From the questions related to self-efficacy of purchasing foods such as whole grains or foods low in fat or sodium, a statement regarding confidence of finding whole grains was scored the highest (mean=3.49) while a statement regarding the confidence to purchase foods that are trans fats free received the lowest scores (mean=3.05). The means and standard deviation for all self-efficacy statements are listed in Table 2.
Beliefs and knowledge statements
The vast majority of participants scored fruits, vegetables, whole grains, flax seeds and nuts as either somewhat healthy or very healthy. Both red and processed meats were scored by most participants as either very or somewhat unhealthy (Table 3). Most participants indicated that diseases such as heart diseases, diabetes, or high blood pressure could be prevented by eating more fruits, vegetables, whole grains, fiber and less total fat, saturated fat, trans fats, cholesterol, sugar, salt or by taking vitamins and/or mineral supplements (Table 5).
Most participants indicated that they either ate some but not enough or that they should eat more of food such as whole grain breads or cereal, fruits or vegetables. The exceptions included both red and processed meats. I should eat less of it/them was the most often picked option for the processed meats category while more then three quarters choose either I should eat less of it/them or My intake is about right for red meat option (Table 4).
Participants had relatively adequate knowledge about the link between food/disease prevention and the nutrient content of specific foods. Eleven out of 20 of the knowledge questions were answered correctly more than 75% of the time (Table 6). Respondents were most likely (96.5%) to be able to identify foods that had the highest content of cholesterol. Respondents were least likely (34.5%) to be able to identify foods that had the highest content of sodium. However, knowledge regarding recommended intake of fruits and vegetables was low with the corrected answers obtained from 17.5% and 16% of participants, respectively.
Discussion
People living in the eastern region of North Carolina have higher rate of obesity, diabetes, cancer and other health problems compared to the rest of the state and to national statistics. Many of these health conditions are a result of unhealthy eating habits that may include high intake of saturated and trans fats, and low intake of fruits, vegetables, whole grains and other healthy foods. The goal of the current study was to assess beliefs, barriers and self-efficacy of eating a healthy diet and self-efficacy of shopping for foods such as whole grains or foods designated as low fat or low sodium. Additionally, assessment of beliefs about healthfulness, appropriate consumption, and protective aspect of specific foods including fruits, vegetables, and whole grains was made.
Participants gave relative low scores for all statements regarding barriers to eating healthy foods except for a statement about the price for buying healthy foods. These scores were also lower than scores regarding perceived benefits. The high value of benefits and somewhat lower value of barriers in this sample were consistent with those reported by Henry et al. (2006) regarding decisional balance scores for fruits and vegetables. Perceived benefits have also been reported as important factors to consider in consumption of fruits and vegetables by people from other studies. Moser et al. (2005) for example, found that intrinsic benefits such as living longer, losing or maintaining weight and having more energy were the best predictors of intakes of fruits. The results of the current study showed that beliefs that the intrinsic benefits of eating a healthy diet such as feeling better or being healthier received the highest scores from all benefits statements. The low scores for barrier statements and relatively high scores for benefits indicate that they saw few obstacles and many benefits to eat healthy. Also, only the cost of healthy foods was considered a significant barrier to eat healthy. Moser et al. (2005) suggested that such intrinsic factors may be helpful in the efforts to increase intakes of fruits among African American males. However, the self-reported perceived intake reported in the current study shows that these beliefs did not translate into perceived increased intakes (Table 4).
Contrary to previously published studies, participants of the current study did not consider dietary preferences of significant individuals such as family members or friends to be significant barriers to eat healthy. Participants included in a sample in the Airhihenbuwa and Kumanyika (1996) study, perceived those with whom food is eaten as a very relevant factor for food preferences. Moser et al. (2005) suggested based on their results that significant individuals such as family or peers would have a significant impact on intake of fruits among African American men.
In spite of the high evaluation of benefits and relatively low score value for barriers most participants indicated that they consumed inadequate intake of foods they indicated as healthy while indicating too high consumption of foods believed to be unhealthful. In the light of the above, the question must be asked why the knowledge and beliefs as well as low value of perceived barriers to eat healthy and high value of perceived benefits do not coincide with the indicated behavior? Ard et al. (2005) found that acculturations are important factors in consumption of fruits, vegetables and the amount of fat. They found that African Americans who were more traditional in their religious beliefs, had preferences for things African American, interracial attitudes, health beliefs and practices, racial segregation, and family values ate fewer servings of fruits and vegetables and more fat. Findings reported by Airhihenbuwa and Kumanyika (1996) also seem to support the influence of culture on food preferences among African Americans. Although participants in that study stated that being black has nothing to do with food preferences, they did state that "Food practices are handed down from generation to generation. Once your body gets used to a particular type of food, it is not easy to switch to another type." They also stated that "I noticed that anywhere Black people go, they do tend to go where the more spicier type food is." Although acculturation was not found to be a significant predictor of fat intake in a sample included in a study by Evans (2007), most research on food preferences of African Americans strongly suggests acculturation to be a very important factor. It is safe to assume that the current results may be explained by the idea that cultural beliefs and attitudes may influence dietary pattern regardless of awareness of disease prevention or beliefs regarding healthfulness of foods. Cultural beliefs are believed to be particularly strong in the southern region of the U.S. and the eastern part of North Carolina which was the setting for the current study and is a part of the U.S. south.
Taste and food preferences were reported in other studies as important predictors of intake of vegetables. Moser et al. (2005) found that preference for foods such as candy, cookies, or ice cream was an important determinant of limited intake of vegetables. The results of Moser et al.'s study were consistent with similar studies that reported taste as a barrier to eating vegetables but not fruits. The results of the previous studies would indicate that taste would be a stronger factor in food selection than awareness of health issues and other perceived benefits or barriers. However, barrier statements related to taste included in our survey did not receive very high scores indicating that they were not very important in food selection (Table 1).
Participants in the current study indicated that both red and processed meats are not healthy and that they should consume less of them. This finding is consistent with the findings reported by Airhihenbuwa and Kumanyika (1996) who interviewed groups of African Americans in a focus group setting. Fourteen participants in that study believed that foods high in fat and saturated fat should be modified or replaced by foods lower in fat. The perceived high consumption of meats reported by the participants of the current study was consistent with other reports. According to Gans et al. (2003), black participants from their sample were less likely to eat meatless meals and modify meats to make them lower in fat. They were also less likely to modify other dietary behavior related to fat intake such as consuming low fat cookies or milk.
Based on ethnicity and weight status the participants included in this study were at high risk for many chronic health conditions. The results showed that overall participants had adequate knowledge about the association of specific foods such as fruits, vegetables, whole grains or processed meats with disease prevention and the nutrient content of specific foods (Table 5). However, only a small percentage of respondents correctly answered questions about recommended intakes of fruits or vegetables. The low rate of awareness about the recommendation for produce is consistent with those reported by Stables et al. (2002). According to their report which was based on a nationally represented sample, just 5.36% and 13.82% of African American respondents surveyed in 1991 and 1997, respectively, were aware of the recommendations for fruit and vegetable intake.
Generally speaking participants gave high scores for perceived benefits (considered them to be important) to eat healthy while barriers of eating healthy received much lower values (considered to be less important factors). Also, participants expressed relatively high self-efficacy of eating healthy foods and purchasing foods that could help them to improve their diets. Additionally, participants showed high awareness of foods that are associated with disease prevention including fruits, vegetables, and whole grains. They also had a good understanding of nutrient content in selected foods. Based on these results, future programs designed to improve diets for this population should not be focused on increasing awareness of benefits of, addressing barriers of healthy eating or to seek to increase self-efficacy of eating or purchasing healthy foods. However, participants did indicate that they do not eat enough of the foods perceived to be healthy and that they eat too much of foods that are known to be unhealthy. Diet plays a very important part of disease prevention and development. Since African Americans are disproportionately affected by many diet related diseases, it is essential that further research be conducted to understand why African Americans have the dietary behaviors they have. One possibility that needs further exploration is the factor of cultural identification on dietary behaviors in this population. In order for interventions to be successful, they must include honest conversations regarding cultural aspects of dietary preferences. Interventions should also focus not only on individuals but entire families and communities at large. In recent years, faith-based health programs have become increasingly popular because of acceptability and positive outcomes especially in African American populations. Church and church leaders can play a very important role in making some desirable changes in food habits of church members. Church based nutrition interventions that include changes in policies regarding healthy foods offered at events, finding opportunities to introduce new healthy foods, and teaching alternative ways of food preparation may be more effective at making lasting dietary changes. Additionally church-based interventions may be even more successful if they include a Biblical foundation for the recommended healthy dietary changes. The Bible plays an important place in the lives of many African American members of Protestant denominations and contains a number of texts, stories and characters that center around food or attitudes of people toward food. For example, Biblical texts can be used to teach about grains, legumes, fruits and vegetables, nuts, flax seeds, honey and olive oil. Additionally, concepts such as variety, moderation, temperance, and self-control can be supported by the scriptures and may be especially important considering that overeating and over nutrition is a primary issue in the development of obesity and thus subsequent chronic health disease. The results of this study could be incorporated into future church-based nutrition interventions with the African American community in the southeast region of North Carolina.




 XML Download
XML Download