

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
The incidence of diabetes, one of chronic diseases, has been increasing every year and the 2/3 of the world's diabetes patients are distributed in developing countries, among which 70% have been reported in the Asia-Pacific areas including Korea (Korea Technology Transfer Center, 2006). If the incidence of diabetes is increased with the present rate, the number of diabetic patients in the world will be increased at least to 2-3 times of the current number by 2025, making diabetes as a worldwide problem. However, it is more serious in case of our country and according to the recently reported results of the National Health and Nutrition Survey of Korea Centers for Disease Control (KCDC, 2009), as of 2007, the number of diabetic patients in the country was 9.5% of the population and the mortality has increased by 11.6% from 13.5% to 25.1% for the past 10 years (Korea National Statistical Office, 2006). Such increase of incidence may result in a serious situation where the number of diabetic patients will be increased to one in every seven people in the population by 2030 (Korea Technology Transfer Center, 2006). In Korea, diabetes is one of the 4 major causes of death following cancer, cerebrovascular disease, and heart disease, and becomes an important problem in the aspect of national public health due to hospitalization caused by diabetes, increase of mortality, and increase of related medical expenses (Lee, 2000).
Complications due to diabetes have become more serious problems than diabetes itself and the development of such chronic complications is closely related to high blood glucose levels. Thus intensive blood glucose control can reduce the mortality of diabetes by decreasing the development of chronic complications. Yet the most important practice for controlling blood glucose in diabetic patients is diet therapy. Diet therapy is a type of treatment to understand abnormal metabolism of nutrients and to figure out and manage the relationship between food intakes and blood glucose levels. For effective blood glucose control, accurate nutrition information and active practice of diet therapy by a patient are required. In addition, understanding for diabetes, providing useful information for patients, and positive support by family members greatly help patients practice their diet therapies. Particularly patients with chronic diseases are very dependent on their family members and are influenced by their attitudes, (Jeong et al., 1985; Kan 1988), and thus family support has been reported to significantly influence the short-term or long-term recovery of patients with chronic diseases (Kaplan et al., 1977). As mentioned above, the close relationship between treatment for diabetes and family function has been confirmed, but education programs for diabetes performed so far have only involved patients and seldom included their family members (Cha, 2004).
Previous studies related to this study have been performed so far mainly in the areas of nursing and social welfare, and the contents of those reported studies included family support and the quality of life of diabetic patients (Cho et al., 2003; Cole & Chesla 2006; Kim et al., 2007), the relationship between family support and diet therapy practice of diabetic patients (Jang 1999; Kang et al., 1995; Kim, 1999; Park 2000), the relationship between family support and blood glucose level (Kim et al., 2007), and diet therapy practice of diabetic patients and blood glucose control (Choi, 2001; Lee et al., 2004). However, the content of diet therapy was not mainly examined in the studies of such areas and some questions on diet therapy practice were partly included while investigating 'self-care performance' or 'compliance with sick-role behavior' (Kang, 2002; Lee 1987; Lee, 2000; Park, 1984). Thus, studies on detailed diet therapy practice or related family support for controlling blood glucose levels in diabetic patients have seldom been performed in the nutritional approach.
Therefore, in this study, the content and degree of family support related to diet therapy and the diet therapy practice of patients themselves were investigated in patients with type II diabetes in the Chungbuk area, and also examined the relationship among such family support and diet therapy practice and blood glucose control, and thus tries to prepare basic data for the development of effective education programs to control blood glucose levels in diabetic patients.
Subjects and Methods
Subjects and study period
The subjects of this study were hospitalized patients or outpatients who visited hospitals because of diabetes. The criteria for the study subjects included both male and female type II diabetic patients who were over 20 years of age, able to communicate, had family members, and the survey was performed for those who could understand the purpose of this study and agreed to participate in the study. The survey questionnaire was constructed by investigators on the basis of previous studies (Gill, 2004; Kang, 2002; Moon, 2004), and the preliminary survey was performed on 30 diabetic patients between March 2 and March 30, 2006, and after modification and supplementation, the main survey was performed for 5 months from April 3 and to August 31, 2006. The self-administered questionnaire was distributed to diabetic patients except the elderly who had difficulties in understanding clearly. In such cases, the investigators read the questionnaire to the elderly patients and wrote down their answers on the questionnaire. Among 86 survey questionnaires collected, 4 copies were excluded due to incomplete answers, and a total of 82 copies were used in the data analysis.
Study content and methods
1) Anthropometric measurements
For anthropometric measurement, the medical records of the patients measured in the hospital were used.
2) Survey questionnaire
Questions for general characteristics included 7 items such as gender, age, marital status, occupation, monthly income, education level, and the number of family members, and questions for diabetes related status included duration of illness, method of treatment, presence of complications, type of complications, number of complications, and experience for exercise and nutrition education. Each of 10 questions were included for family support related to diet therapy practice and the patient's diet therapy practice, which were all measured by the Likert 4-point scale. For the reliability of the survey questionnaire, Cronbach's a coefficient was calculated, and family support items showed 0.85-0.93 and diet therapy practice items showed 0.83-0.90.
3) Classification of the subjects based on blood glucose control
Among the subjects who answered to practice diet therapy, supervising physicians evaluated the degree of controlling blood glucose levels of individual diabetic patients and classified to 3 groups (excellent, fair, poor) on the basis of medical records during the 2-month treatment period.
Data analysis and statistical analysis
The frequency and percentage for each survey question were calculated, and scores for family support and diet therapy practice were given by using the Likert scale with 4 points for 'strongly agree', 3 points for 'agree', 2 points for 'disagree', and 1 point for 'strongly disagree', and then the mean and standard deviation were obtained. For questionnaire items for family support and diet therapy practice, the results according to the factor analysis by Varimax rotation method showed that items for family support were not derived as factors, but two factors (control of food intakes, restriction on specific nutrients) were derived from items for diet therapy practice. The χ2-test, ANOVA and Pearson's Coefficient were calculated to examine the relationship between family support, diet therapy practice score, and blood glucose control. Among 82 survey questionnaire used for the analysis, 67 copies answered for diet therapy, which were thus used for the verification of statistical significance. For statistical analysis, SAS 8.2 program was used.
Results
General characteristics of the subjects
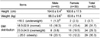
The general characteristics of the subjects are listed in Table 1. The gender distribution of subjects was 52.4% males and 47.6% females, and the age distribution was high in 50-59 years (43.9%), and 79.3% were married. The occupation included housewife (23.2%), sales (20.7%), and agriculture (15.8%), and the monthly income distribution was the highest at one million won and below as 53.7%. For education levels, high school graduates (34.2%) was the highest, and the number of family size was the highest at 4~5 (45.1%).
Diabetes related status of the subjects
1) Anthropometric measurements
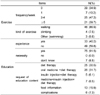
The average height and weight of 82 subjects were 164.6 cm and 66.0 kg in males and 160.8 cm and 63.8 kg in females, respectively, and BMI (Korean Society for the Study of Obesity, 2005) was 18.5-22.9 (31.7%), 23.0-24.9 (29.3%), and over 25.0 (35.3%) (Table 2).
2) Diabetes profiles
Diabetes profiles are presented in Table 3. The average duration of illness of the subjects was 8.4 years and 81.7% (n=67) of the 82 subjects answered diet therapy as current diabetes treatment. For the experience of complications due to diabetes, 42.7% answered 'yes' and the type of complications in subjects obtained from multiple responses were highest in the order of retinopathy (26.1%), peripheral neuropathy (23.9%), renal disorders (10.9%), and heart disease (10.9%), showing the highest frequency of retinopathy among diabetes complications. At the present time of the study, 62.2% had no complications and 37.8% had more than one complications.
3) Exercise and diabetes education related status (Table 4)
Among 82 subjects in this study, 34.9% never exercised and 65.1% exercised. The frequency of exercise showed the highest at 2-4 times/week (47.2%) and then over 5 times/week (39.7%), and the type of exercise was the highest in walking (86.9%).
40.2% of the subjects experienced diabetes education and 91.5% answered that diabetes education was necessary. For desirable contents of nutrition education, 76.8% of the subjects wanted diet therapy, among which oral medicine along with diet therapy (31.7%) and diet therapy only (30.5%) were high.
Relationship between family support and blood glucose control
1) Family support
As presented in (Fig. 1), the content and degree of family support showed that questions with higher family support (strongly agree + agree) included 'advice for regular meals' (82.1%) and 'cooking by considering restricted foods' (71.5%), and questions with lower family support included 'advice for practicing diet therapy while eating out' (44.8%) and 'collection and delivery of information on diet therapy' (46.3%).
2) Relationship between family support and blood glucose control
Based on the evaluation of blood glucose control by supervising physician, 29.9% (n=20) of the 67 subjects who answered practicing diet therapy were classified to "excellent", 38.8% (n=26) "fair" and 31.3% (n=21) were "poor" (Table 5). The family support scores of three groups according to the degree of blood glucose control showed that family support score of a group with 'excellent' blood glucose control was higher than those of groups with 'fair' or 'poor' control in 8 out of 10 questions on family support (Table 5). Among them, 'cooking by considering restricted foods' showed the greatest difference between groups (p<0.001). Also, the correlation by Pearson's Coefficient between all family support scores and blood glucose control showed high correlation (r=0.341, p=0.0002).
Relationship between diet therapy practice and blood glucose control
1) Diet therapy practice
Ten question items for diet therapy practice were asked to 67 subjects who answered practicing diet therapy and the results showed that questions with positive responses (strongly agree+agree) included 'restriction on taking simple sugars' (74.6%) and 'trying to take dietary fibers' (70.1%), while questions with lower diet therapy practice included 'restriction on food intakes while eating out' (32.9%) and 'control of meal intake according to exercise' (38.8%) (Fig. 2).
2) Relationship between diet therapy practice and blood glucose control
The diet therapy practice scores of the three groups according to the degree of blood glucose control (Table 6) showed that the score of a group with 'excellent' blood glucose control was higher than other groups in all of 10 question items. Also, the correlation by Pearson's Coefficient between diet therapy practice and blood glucose control showed high correlation (r=0.304, p=0.0007).
Other factors related to blood glucose control
The results of χ2 test for identification of other factors affecting blood glucose control, showed that gender, age, monthly income, education level, number of family members, BMI, and exercise frequency were not related to blood glucose control, but only the experience of diabetes education was related to blood glucose control (Table 7). The rate of excellent blood glucose control in subjects who received diabetes education was 46.7% while that in subjects with no nutrition education was 16.2%, demonstrating significantly excellent blood glucose control in groups with diabetes education compared to groups without education (p<0.05).
Discussion
In the content and degree of family support of diabetic patients examined in this study, the question with highest family support was 'advice for regular meals' (82.1%) and the questions with lower family support were 'advice for practicing diet therapy while eating out' (44.8%) and 'cooking at home by diet therapy' (50.7%). These results were similar to those from the study by Kim (1999), in which the question item with highest family support was 'advice when skipping the meals', suggesting that family members generally cooperate diabetic patients to keep their meal time. Results from these two studies were similar in question items with lower family support, and the lowest question was 'cooking by family members considering diet therapy'. Also, in the study of Kang et al. (1995), the lowest score came from the item 'family members always prepare the meal based on food exchange table for diabetics'. From the above study results, it is considered that sufficient education on cooking methods based on the food exchange table is needed for family members who prepare meals for diabetic patients during the diabetes education.
Studies about the influence of family support on blood glucose control of diabetic patients have been rarely performed until now. Among reported studies, Kim et al. (2007) showed no significant correlation between family support scales and blood glucose levels but a significant relationship between some of sub-scales and postprandial (2 hr. after meal) blood glucose level, suggesting family support as an important factor in blood glucose control of diabetic patients. In this study, the results of family support scores of the three groups according to the degree of blood glucose control to examine the relationship between family support and blood glucose level showed that the family support score of a group with 'excellent' blood glucose control was higher than those of groups with 'fair' or 'poor' control in 8 out of 10 questions on family support. Also, the correlation by Pearson's Coefficient between all family support scores and blood glucose Control showed high correlation (r=0.341, p=0.0002). This means that family support can influence blood glucose control of diabetic patients.
For the degree of diet therapy practice of diabetic patients themselves, question items with higher degree of practice were 'restriction on taking simple sugars' (74.6%) and 'trying to take dietary fiber' (70.1%), while questions with lower degree of practice were 'restriction on food intakes while eating out' (32.9%) and 'control of meal intake according to exercise' (38.8%), demonstrating that the practice rate of restriction for specific nutrients was high but that for controlling food intakes during eating out or exercise was very low. In the studies of Yoo (1988) and Lee (2000), patients restricted their favorite foods or beverages to some degrees by themselves but showed the lowest score on the question item 'control of food intake by oneself using food exchange table', which was similar to the result of this study showing the lack of ability of patients to control their food intakes by themselves. On the other hand, Lee et al. (2004) investigated the influence of diabetes education on diet therapy practice of diabetic patients, in which keeping food intakes and the use of food exchange table were significantly higher among diet therapy practices after diabetes education, and the degree of diet therapy practice became higher particularly when the practice through diabetes buffet was additionally provided (Lee & Lee, 2007), demonstrating the importance of diabetes education in the practice of diet therapy of diabetic patients.
For the relationship between diet therapy practice of diabetic patients and blood glucose level, the diet therapy practice scores of the three groups according to the degree of blood glucose control showed that the score of a group with excellent blood glucose control was the highest in both of two factors (control of food intakes, restriction on specific nutrients) of diet therapy contents (p<0.001), and showed significantly higher practice scores in 9 out of 10 question items for diet therapy practice. In particular, question items such as 'restriction on taking simple sugars', 'trying to take dietary fibers' and 'keeping food intakes' showed much higher practice scores in groups with excellent blood glucose control than those in groups with fair or poor control (p<0.001). Also, the correlation by Pearson's Coefficient between diet therapy practice and blood glucose control showed high correlation (r=0.304, p=0.0007). From the above results, diet therapy practice are known to affect the blood glucose control of diabetic patients, but unable to compare with other study results because no previous studies that can be directly comparable were found.
For other factors affecting blood glucose control, a group which received diabetes education showed better results in blood glucose control than groups without education (p<0.05). There are many studies on the effects of diabetes education, among which the study of Lee et al. (2004) showed significantly higher scores in 8 question items such as the necessity of diet therapy after diabetes education, principles of diet therapy, nutrient composition of foods, carbohydrate content of foods, prescribed daily calorie, food exchange unit for the prescribed calorie, exchange unit for grain group, and exchange for fruit group. In addition, postprandial blood glucose level at 2 hours after the meal was significantly decreased after diabetes education (p<0.001). Also, in the study about the effect of nutrition counseling on blood glucose and diet of patients with type II diabetes (Lee & Lee, 2007), the fasting and postprandial blood glucose levels were significantly decreased after nutrition counseling on diabetes. Also, Choi (2001) reported that a negative correlation between glycosylated hemoglobin and the number of diabetes education, suggesting that diabetes education helps blood glucose control, and the effect of diabetes education on blood glucose control is also confirmed in this study. However, for the experience of diabetes education of subjects in this study, about 60% of the subjects had no experience of diabetes education and 91.5% of the subjects answered that nutrition education for diabetes control is necessary; suggesting that even subjects who had no experience of diabetes education strongly felt its necessity.
The exercise status of subjects in this study showed that 65.1% exercised and 34.9% never exercised. This exercise rate is higher than 51.3% in the study of Park et al. (1988) and 56.3% in the study of Choi (2001) but lower than 74.2% in the study of Kim (2002). The type of exercise showed the highest rate in walking (86.9%) and the frequency of exercise was the highest at 2-4 times/week (47.2%) and then over 5 times/week (39.7%). In particular, because diabetic patients using insulin have fewer chances for complications and longer healthy life if exercise regularly, it is necessary to educate patients to exercise regularly for the prevention of complications and the management of diabetes exercise. In the study of Lee et al. (2004) in which changes of exercise habits were measured in diabetic patients after diabetes education, the frequency of exercise was significantly increased after education and the degree of obesity was significantly decreased, and body weight, systolic blood pressure, and diastolic blood pressure tended to be decreased. Also in another study (Lee & Lee, 2007), the frequency of exercise was significantly increased after nutrition counseling on diabetes (p<0.01), suggesting that it is necessary to include exercise in diabetes education for proper diabetes management. In this study, it was also expected that exercise would give positive influence on blood glucose control, but these two factors were not related. It is thought that it was unable to perform detailed analysis because only the type of exercise and the amount of exercise per week were examined in the study and the intensity and duration of exercise were not studied. Thus it is necessary to perform more detailed investigation on exercise in diabetic patients and to analyze the relationship with blood glucose control in future research.
From the above results, it has been known that blood glucose control of diabetic patients is greatly influenced by family support, diet therapy practice, and the experience of diabetes education. Therefore, measures to increase family support of diabetic patients should be prepared for the improvement of blood glucose control in diabetic patients. However, to be realistic, the percentage of patients who received diabetes education was about 40% in this study, and the percentage of family members participating in diabetes education was as low as 18.4% (Kim et al., 2007), it is urgently needed to develop and expand the contents of diabetes education programs including not only patients themselves but also their family members. Thus on the basis of these results, it is suggested that the contents such as the control of food intakes during eating-out or exercise, the necessity of exercise, the intensity of exercise and the amount of exercise per unit time should be included for patients themselves, and the contents such as cooking practice using food exchange table, overall diet therapy and drug therapy(including insulin therapy) should be included for family members.







 XML Download
XML Download