

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Metabolic changes associated with ingestion of different contents of macronutrients in a diet may contribute to the development of diseases including type 2 diabetes, cardiovascular disease (CVD) and obesity (Mcgregor & Lee, 1995; Sargrad et al., 2005; Shai et al., 2008). Low carbohydrate diets (for a decrease of 90 g/d) have been suggested to be beneficial in the treatment of the metabolic syndrome (Volek & Feinman, 2005). One meta-analysis showed that low carbohydrate diet that provided less than 45% of energy from carbohydrates resulted in good glycemic control within 6 months when it was substituted for a conventional high carbohydrate diet in patients with type 2 diabetes (Gougeon et al., 2006).
Altered contents of carbohydrate or fat in the meal affect the hepatic enzymes that metabolize carbohydrate or fat as substrates (acyl-CoA synthetase, carnitine palmitoyl-transferase-1 and acetyl-CoA carboxylase) in animal study (Ryu & Cha, 2003). Clinical studies support that diets rich in carbohydrate can lead to elevation in fasting plasma triglyceride (TG) as a result of hepatic very low density lipoprotein (VLDL) and chylomicron remnants accumulation due to altered lipoprotein secretion and/or clearance (Lopez-Miranda et al., 2007; Park et al., 1999). In addition, dietary carbohydrates may affect insulin action, at least in part, via alterations in plasma free fatty acids (Coulston et al., 1983).
The extent and kinetics of such postprandial changes are highly variable and modulated by numerous factors such as dietary patterns, meal composition and several lifestyle conditions (physical activity, tobacco use) (Lopez-Miranda et al., 2007).
Although a few studies reported influences of typical Korean diet on postprandial macronutrient metabolism in normal subjects (Yoon & Kim, 1998) or diabetic patients (Kwon & Kim, 2003), blood kinetics associated with different macronutrients composition in the meal had not been clearly determined in healthy Korean women.
In the present study, we compared the kinetic effects between isoenergetic high carbohydrate and high fat meals on blood glucose, insulin and lipids in normoglycemic and normolipidemic Korean women. One of the diets was higher in carbohydrate (75% vs usual 55-70%), the other higher in fat (61% vs usual 15-25%) and both were similar in protein, than the acceptable macronutrient distribution ranges in Korea.
Subjects and Methods
The protocol for this clinical research was reviewed by the Institutional Review Board (IRB) at the Kyung Hee University Medical Center (Seoul, Korea).
Sample
Healthy young women were recruited on the university and hospital employee announcement boards. Eligibility criteria included willingness to participate the study protocol, and understanding and signing of informed consent; being diagnosed as normal weight (BMI<23 kg/m2), fasting blood glucose concentrations of less than 100 mg per 100 ml, no report of abnormal blood glucose level within the last half year; and being aged over 20 years.
Exclusion criteria included any serious complicated diseases and medication. Thirty subjects were screened and enrolled, however, 5 subjects dropped out because of personal and technical problems. The final number of study subjects was 25.
Using a stratified randomization procedure, thirteen subjects were assigned to the high carbohydrate meal (HCM) group, twelve to the high fat meal (HFM) group. Subjects were maintained fasting state for 12 h before they ingested test diets. Severe physical activity and heavy drink of alcohol, caffeine, green tea or supplements were not allowed before the study.
Test meals
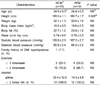
Two test meals as the typical Korean menu were prepared by a certified cook; steamed-rice, mushroom soup with soy paste, Deonjang, grilled marinated-pork with pepper paste, Gochujang, vegetable salad with boiled egg white, and Kimchi. Total energy provided by each test meal was approximately same as 600 Kcal (Table 1). Carbohydrate and fat modification consisted of a meal based on the amount of steamed-rice and salad dressing. Each contained 15% of calories from protein. The high carbohydrate meal composed of 111.7 grams of carbohydrate (75.0% of calorie derived from CHO) and high fat meal composed of 40.6 grams of fat (61.1% of calorie derived from fat) (Table 1). The subjects were advised to consume each meal over a 15 min period.
Measurements
Body weights were measured on a calibrated electronic scale. Body composition was measured by bioelectrical impedance analyzer (Inbody 4.0, Korea). Habitual intakes of nutrients and the ratios of carbohydrate: protein: fat of all subjects were estimated by 3-d food records using CAN Pro version 3.0 (Computer aided nutritional analysis program, Korean Nutrition Society, 2005).
Blood pressure was measured by a standard electronic device (FT500, Korea). Concentrations of blood glucose, plasma insulin, triglyceride and free fatty acids were determined on the fasting, 30, 60, 90, 120, and 240-min blood samples. Blood glucose, triglyceride, plasma fatty acids were determined enzymatically using a Bayer kit (Bayer, USA). Serum insulin was analyzed with a radioimmunoassay kit (Diagnostic products Co.). An estimation of insulin resistance was calculated using the homeostasis model analysis-insulin resistance (HOMA-IR) using the formula: glucose (mmol/L)×[insulin (µU/L)/22.5] (Mattews et al., 1985).
We used the modified quantitative insulin sensitivity check index [QUICKI; 1 / (log(fasting insulin µU/mL) + log(fasting glucose mg/dL)] (Katz et al., 2000; Laaksonen et al., 2005) which was measured from the fasting blood samples that were taken at the beginning of the blood kinetics. As a measure of early phase insulin secretion, the modified insulinogenic index (IGI) was calculated as the ratio of the increment of serum insulin 30 min after the first meal ingestion, to blood glucose concentration 30 min the first meal ingestion after divided by the corresponding increment in glucose [(30 min insulin - fasting insulin) / 30 min glucose] (Wareham et al., 1995).
Statistical analysis
All statistical analyses were conducted using the SAS software package (Version 9.1, SAS Inc., Cary, NC). Continuous variables were presented as mean and standard deviation. Categorical variables were presented as absolute and relative frequencies. The chi-square test was employed to examine the effects of dietary diversity on categorical variables, and continuous variables were compared using the t-test. Statistical significance was accepted within P<0.05.
Results
Demographic characteristics of the subjects
There were no significant differences on the anthropometric measures between the HCM group and the HFM group except the height as shown in Table 2. Majority of the subjects exercised less than 2 times per week (76.9% of HCM and 66.7% of HFM) and all of the subjects drank alcohol less than 2 times per week (100% of each group).
Habitual intake of nutrients
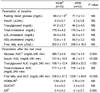
The daily intake of energy and other nutrients at baseline did not differ significantly between the groups as shown in Table 3. In detail, their average usual diet consisted of 68% carbohydrate, 15% protein and 17% fat, which were within the range of Korean dietary composition recommendation, 55-70% carbohydrate, 15-20% protein and 15-25% fat. Mean total energy consumption in current study participants was 1780.2 kcal/d, which does not meet 2,100 kcal/d, the estimated energy requirements (EER) of the Korean Dietary Reference Intake (KDRI) value for 20-y-old women. The groups had no significant differences in food habits such as meal speed, regularity of dietary intake, frequency of daily snack, kinds of snacks, and frequency of eating out (data not shown).
Clinical parameters
Fasting plasma levels of glucose, insulin, triglyceride (TG), and lipoproteins at baseline were all in the reference ranges and not significantly different between the groups as shown in Table 4. After consumption of test meal, relatively higher areas under the curve (AUC) for glucose and insulin were shown in the HCM group than those in the HFM group (P<0.01) (Table 4). No difference was shown for total cholesterol (TC) AUC, however, TG AUC and free fatty acid (FFA) AUC were significantly greater after consumption of HFM (P<0.01). HOMA-IR and the QUICKI insulin sensitivity index did not differ significantly between the groups (Table 4). The IGI was greater in the HCM than in the HFM (P<0.01).
Fig. 1 shows that the HCM group had much higher blood glucose responses at individual time points during the 4 h compared with the HFM group (P<0.01). Similarly, the relative changes in serum insulin responses after consumption of two different test meals were differed significantly between the groups (P<0.01). On the contrary, the blood responses of TG and FFA during 240 min were greater in the HFM group than in the HCM group (P<0.01). No significantly different responses in the serum concentrations of total cholesterol (TC), LDL- and HDL-cholesterol between the groups were presented (Data not shown).
Discussion
Since most studies reported moderate- or long-term effects of different composition of macronutrients in the diet rather than the acute effects on blood kinetics, it is not easy to discuss our results comparing with previous studies (Coulston et al., 1983; Gougeon et al., 2006; Laaksonen et al., 2005, Shai et al., 2008). However, our results are comparable to preliminary evidence that postprandial carbohydrate utilization was increased directly after the administration of a meal or single oral glucose (Liu et al., 1983).
In Chinese subjects, Liu et al. (1990) observed the fasting plasma glucose, insulin and lipids responses to the high-carbohydrate (CHO 80%) and the high-fat diet (Fat 45%). The high carbohydrate diet increased the fasting plasma glucose levels on day 1 (P<0.01), insulin (P<0.01) on day 3 and TG levels on days 3 and 5. On the other hand, the high fat diet decreased plasma TG values on day 1 but increased TC on days 1 and 3, but the fasting plasma glucose levels were decreased slightly on day 5 without a significant difference in insulin levels.
In healthy American volunteers, two levels of dietary carbohydrate (40% and 60% of calorie) consumption for 10 days resulted in that no differences were observed in fasting plasma glucose or cholesterol concentrations. However, fasting plasma TG levels as well as insulin were significantly elevated in the 60% carbohydrate diet group, and HDL-cholesterol concentrations were decreased significantly (Coulston et al., 1983). It is therefore that the levels of dietary carbohydrate may influence the blood measures of lipids, lipoproteins, and insulin which are associated with incidence of coronary heart disease.
Several studies have shown that the amount and nature of carbohydrate in a meal alter postprandial lipid metabolism. Since we compared the influences of relative amounts of macronutrients in the same menu, the latter could not explain our results. Plasma TG concentration was significantly elevated according to the amount of fat consumption (Lopez-Miranda et al., 2007). Some studies using a very low (5 g) or low (15 g) dose of dietary fat did not significantly increase triacylglycerolaemia postprandially; moderate doses (30-50 g) dose-dependently increased postprandial triacylglycerolaemia (from 0.9 to 1.3 mmol/L above baseline, respectively); and very high doses (80 g and above) exaggerated postprandial triacylglycerolaemia but without dose-dependence (Dubois et al., 1998; Lopez-Miranda et al., 2007).
Data obtained after the addition of glucose (50 g, 100 g) to high fat meal have not shown consistent findings on postprandial lipid metabolism in healthy subjects (Cohen & Berger, 1990), whereas the addition of sucrose or fructose has consistently been shown to increase postprandial triacylglycerolaemia (Grant et al., 1994). Therefore, the amount of fat (40.6 g) in the present study was appeared to be enough to stimulate postprandial triacylglycerolaemia, although it is not the usual amount of fat in typical Korean menu. Moreover, the high fat meal was acceptable in the present subjects. All subjects consumed the given menu entirely in recommended time. We found that salad dressing is an easily applicable food item to modify fat consumption in this study.
In healthy subjects, physiological ranges of postprandial hyperglycemia and hyperinsulinaemia as generated by starch foods (bread, pasta, beans) did not induce noticeable alterations in the overall postprandial TG response (Harbis et al., 2004). Similarly, the experimental menu, high carbohydrate meal used in the present study did not altered postprandial TG response. On the other hand, the third National Health and Nutrition Examination Survey (NHANES III) showed that the quantity and type of carbohydrate consumed in the habitual diet did not contribute to the plasma glucose, serum insulin concentration but inversely associated with serum C-reactive protein (CRP) concentration (Yang et al., 2003).
The IGI is a commonly used measure of early insulin secretory capacity (Laaksonen et al., 2005). This index had moderately high correlation with acute insulin responses that were measured during a frequently sampled intravenous glucose tolerance test (r=0.47-0.61). Sharman et al. (2004) showed that the short-term hypoenergetic low-fat diet was more effective at lowering serum LDL-C, but the very low carbohydrate diet was more effective at improving characteristics of the metabolic syndrome as shown by a decrease in fasting serum TG, postprandial lipidemia, serum glucose and greater weight loss.
There are several limitations of the current study. A single diet is a poor descriptor of a person's usual intake, because of individual variability. Also, our results must be considered preliminary due to the small number of study subjects. However, there is widespread interest in "high fat diet" and "high protein diet" alternatives to the conventional "high carbohydrate" approach for weight loss recently. Although a diet low in saturated fats and rich in whole grains, vegetables and fruit is recommended in order to reduce the risk of obesity, cardiovascular disease and type 2 diabetes (McAuley et al., 2005). It is unclear exactly how postprandial glycemia or lipaemia impacts on pathophysiologic conditions such as atherosclerosis, diabetes, and coronary heart diseases. Further studies are expected to investigate the effects of amounts and types of macronutrients in the habitual Korean diets on postprandial response.
In the current study, hyperglycemia and hyperinsulinemia were both induced significantly and acutely by the high carbohydrate meal not by the high fat meal, while gradual hypertriacylglycerolaemia was observed by the high fat meal not by the high carbohydrate meal. In conclusion, macronutrients content in the meal may be an important determinant of postprandial substrate utilization in healthy young individuals.



 XML Download
XML Download