

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
During the past two decades, the role of care as an input into child health and nutrition alongside with food security, availability of health services and healthy environment has been the focus of investigation. Nutritionally, care encompasses all behaviours and practices at the household level of those who give care to children (caregivers), translating available food and health care resources into a child's growth and development. Care is therefore manifested in the ways a child is fed, nurtured, taught and guided (Engel et al., 1997). The significance of care in child nutrition has been articulated in the UNICEF's framework for analyzing the causes of malnutrition among young children in developing countries. The framework suggested that not only were food security and health care services necessary for child survival, growth and development, but care for women and children was equally important (UNICEF, 1990; UNICEF, 1998). The document argued that food, health and care are all necessary, but none alone is sufficient for healthy growth and development. Research has shown that even when there is adequate food in the house and a family lives in a safe and healthful environment and has access to health services, children can still be malnourished (Berggren & Wray, 2002; Mackintosh et al., 2002). It is also believed that even when poverty causes food insecurity and limited health care, enhanced care giving can optimize the use of existing resources to promote good health and nutrition in women and children (Engel et al., 2000). These assertions bring to the fore the need for further investigation of the importance of care in child health and nutrition.
In Ghana and many other developing countries, the problems of malnutrition are considered in terms of household food security without recognition of the important role care or any other factor may play in good nutrition. As a result, other complementary elements of good nutrition have not been captured into efforts of combating childhood malnutrition. This is largely due to a lack of adequate knowledge of their relevance and usefulness in nutritional well-being in these countries. Although the quality of care provided by a caregiver has been conceptualized to have significant effect on child nutritional outcome, only one study has actually assessed the quality of caregiving and child nutritional status in Ghana. In their study of care practices in Accra, Ruel et al. (1999) reported a strong association between caregiver quality of care practice and child nutritional status. This one study, undertaken in an urban community, does not provide adequate information to support the generalization of the possible role of care in child nutrition in Ghana. There is therefore the need to explore the association between quality of care practice and child health and nutrition outcomes, especially in rural communities in Ghana.
In this study, quality of care practice indicators was assessed in terms of household and personal hygiene practices, child immunization status, child dietary diversity, caregiver responsiveness as well as hygienic practices related to feeding using a modified version of the usual positive deviance approach. The term 'positive deviance' has been used to describe the performance regarding health, growth and development of certain children vis-à-vis the performance of other children in the community and the family. From the perspective of young child nutrition therefore, positive deviants are children who grow and develop adequately in low-income families living in impoverished environments, where majority of the children suffer from growth retardation and malnutrition (Zeitlin et al., 1990). This study is based on the premise that differences in caregiving practices may account for differences in nutritional status of children from similar backgrounds and thus similar levels of household resources. Caregiver is defined in this study as the mother or the most responsible person present during the time of observation.
Subjects and Methods
Study site and subjects
The study was conducted in four communities in the Manya Krobo District in the Eastern Region of Ghana. The district is situated about 85km northeast of the capital, Accra, on Longitude 0℃ and Latitude 6° 15' north of the equator. The inhabitants are predominantly from the Krobo ethnic group with a few migrant fishermen and farmers from other tribes. The study population consisted of all mothers with children between the ages of 6 and 12 months. In determining sample size, the following formula which will give an acceptable level of precision for the study was used. Sample size n = t2 × p(100-p) / d2 where t = 2 and is the normal deviate at the required confidence level of 95%, p is the percent rate of variable, which in this case is the estimate of percent of mothers with children between 6 and 12 months (50%); and d is the largest acceptable error in the estimate (10%) (FAO, 1990). Based on this, a sample size of 100 was obtained.
Visits to Maternal and Child Health Centers at Kpong and surrounding villages were conducted to identify mothers with children within the required age group and the objectives of the study were explained to them. Recruitment for participation in the observational study was based on satisfying the following criteria: a) caregivers with infants between 6 and 12 months; b) willingness of caregiver to participate in the study and c) availability of caregiver throughout the observation period. The total number of mothers with children within the desired age range in the population was 400. For caregivers meeting these criteria, separate lists were compiled for both male (198) and female (202) children and every third child on each list was picked to obtain 50 males and 50 females, to ensure gender parity. One hundred mothers with infants between the ages of 6 and 12 months were thus selected for a six-month observational study on quality of care and child nutritional outcome. This age group was chosen because it is most vulnerable period to growth faltering, malnutrition, morbidity and mortality.
Training of field workers
In preparation for the six-month longitudinal data collection, field workers were trained for 2 weeks and standardized on each aspect of behaviour to be observed through home visits. Standardization was carried out until concordance between field workers and their supervisor was obtained. In all, five field workers were trained. To reduce reactivity on the part of caregivers, observations were conducted only after households had been contacted on several occasions. Each observer was assigned to twenty households, which they consistently observed throughout the observation period.
Data collection methods
Each child received one behavioral observation visit per month, for a period of six months. At each home visit, data were collected on household and personal hygiene practices, child's immunization status, child's dietary diversity, caregiver responsiveness as well as hygienic practices during feeding using a combination of methods. Child anthropometry was also collected monthly over the six month period.
Assessment of quality of care practice indicators
Indicators of quality of care used in this study were household and personal hygiene practices, child's immunization status, child's dietary diversity, caregiver responsiveness and hygienic practices during feeding. Caregiver household and personal hygiene practices were assessed using spot check observations. For caregiver hygienic behaviours, nine hygiene-related aspects were examined. These included cleanliness of house, presence of human and animal faecal matter, stagnant water and open garbage containers on the compound. Others were general appearance of caregiver and index child, buttocks of index child being fully covered and the presence of unwashed cooking/eating utensils. Each positive behaviour (eg child clean) received a value of 1 and a negative behaviour (eg. unclean house), a value of 0. Thus, the maximum hygiene score one could obtain on each visit was 9 and a minimum of 0. At the end of the study, mean hygiene scores were computed and quartiles generated based on their frequency distribution. Individuals with scores below the 25th quartile were classified to have poor hygiene practice; those between 25th and 50th quartile as having an average hygiene practice; 50th to 75th quartile as having good hygiene practice and those above 75th quartile as of very good hygiene practices.
In assessing child immunization status, the child's weighing card (health record card) was collected during each visit and information on all vaccines received noted. At the end of the study, the child's immunization status was determined based on completeness of each of the four major vaccines (i.e. poliomyelitis, DPT, measles and yellow fever). Children who had not received any of the vaccines were classified as having no immunization status in terms of that particular vaccine. For polio and DPT, children who had received less than three shots were classified as being of incomplete status and those with three or more as having complete status. With measles and yellow fever, the classification was either no immunization or complete immunization, respectively for those who had not received the vaccines and those who had. In assessing the overall immunization status of the children, a score of 0, 1 and 2 were assigned to no immunization, incomplete immunization and complete immunization respectively. The maximum overall immunization status score one could obtain based on polio, DPT, measles and yellow fever was 8 and a minimum of 0.
Dietary diversity score, defined as either the total number of foods consumed or the total food groups consumed by Hatløy et al. (2000) has been reported to be a useful indicator of dietary quality. Food groups based on the usual child feeding and consumption patterns in Accra reported by Amar-Klemesu and Ruel (2000) was adopted, modified and used to assess dietary diversity. The groups used were: 1) cereal and cereal products; 2) roots, tubers and plantain; 3) meat products; 4) fish and sea foods; 5) eggs; 6) milk and milk products; 7) margarine; 8) legumes, nuts and pulses; 9) fruits; and 10) soups and stews. A score of 1 was assigned to any food group consumed and 0 when it was not consumed. The highest score a child could obtain on each visit was therefore 10. Mean dietary diversity scores for each child over the period were computed and divided into quartiles based on their frequency distribution. Individuals with scores below the 25th quartile were classified to have poor dietary diversity; those between 25th and 50th quartile as having average dietary diversity; 50th to 75th quartile as having good dietary diversity and those above 75th quartile as of very good dietary diversity.
Caregiver responsiveness during feeding was assessed through direct observation as to whether the caregiver exhibited any of the following behaviours; encouraging the child to eat, demonstrating to child how to eat, offering more food to child, talking to child whilst eating, supervising child feeding, monitoring how much child eats, and not ordering or threatening child to eat. Each positive behaviour (e.g. 'offers more food') received a value of 1 and a negative behaviour (e.g. 'orders child to eat'), a value of 0. At the end of the study, mean scores were computed and quartiles generated based on their frequency distribution. Individuals with scores below the 25th quartile were classified to have been poorly responsive; those between 25th and 50th quartile as being averagely responsive; 50th to 75th quartile as showing good responsiveness and those above 75th quartile as exhibiting very good responsiveness.
Caregiver hygienic practices during feeding was assessed in terms of caregiver washing own hands and child's hands during and after feeding, using clean feeding utensils, keeping feeding area clean, use of clean water and soap to wash hands, washing both hands, rubbing hands together at least 3 times and drying hands using clean cloth/towel. Each positive behaviour (e.g. 'uses soap') received a value of 1 and a negative behaviour (e.g. 'does not use clean water'), a value of 0. Mean scores were computed and quartiles generated based on their frequency distribution. Individuals with scores below the 25th quartile were classified to have poor hygienic practices; those between 25th and 50th quartile as having average hygienic practices; 50th to 75th quartile as showing good hygienic practices and those above 75th quartile as showing very good hygienic practices.
Mindful of the fact that no single indicator can capture the complex patterns of behaviour that constitute good child care practice, we created a quality of care index to take into consideration the care indicators measured using the mean score of the following care indicators; a) household and personal hygiene, b) overall immunization status, c) dietary diversity, d) caregiver responsiveness and e) hygienic practices during feeding. Quartiles were generated based on frequency distribution of the overall quality of care index. Individuals with values below the 25th quartile were classified to have exhibited poor quality of care practice; those between 25th and 50th quartile as having shown an average quality of care practice; 50th to 75th quartile as showing good quality of care practice and those above 75th quartile as exhibiting very good quality of care practice.
Identification of child nutritional status (positive and negative deviant children)
Weights and lengths measurements of the children were taken monthly for a period of six months. Monthly weight-for-age (WAZ), length-for-age (LAZ) and weight-for-length (WLZ) z-scores were generated using WHO (1983) reference. At the end of the study, the mean z-scores were computed for each child. The children were then classified as positive deviants or negative deviants based on their attained weight-for-age and length-for-age z-scores. The z-scores were averaged over the 6-month period to give a good reflection of the cumulative effect of care over that period of time on child nutritional status. Positive and negative deviance in child nutrition has been defined by Shekar et al. (1991) as growth that is below or above the norm of a population. This norm has been defined primarily based on anthropometric growth compared to acceptable standards. Whishik and Van der Vynckt (1976) also proposed the threshold concept for classifying nutritional positive deviants. The threshold establishes a point of simple dichotomy into two groups, those above and those below that point. For our study, in classifying the children, the median WAZ and LAZ were taken as the norm of the population and thus the threshold. Thus the requirements were for the child to be above the threshold both according to his WAZ and LAZ. With either one below the threshold, the child was placed in the lower nutritional group. Children with both WAZ and LAZ above the median WAZ and LAZ of the group were classified as positive deviants and the rest as negative deviants. Based on this classification, 34 children were identified as positive deviants and 66 as negative deviants. Since the classification was done at the end of the study, the observers were not aware of the status of the children to begin with.
Data analysis
Results were analyzed using Statistical Package for Social Sciences (SPSS) Version 10 in Windows. Means and standard deviations were generated for continuous variables and frequency distributions for categorical variables. Statistical significance between positive deviants and negative deviants was tested using the independent t-test for continuous variables and the chi-squared test for categorical variables. The multiple regression analysis was used to explore how the various care indicators actually predicted a child's nutritional status, with child deviant status being the dependent variable.
Results
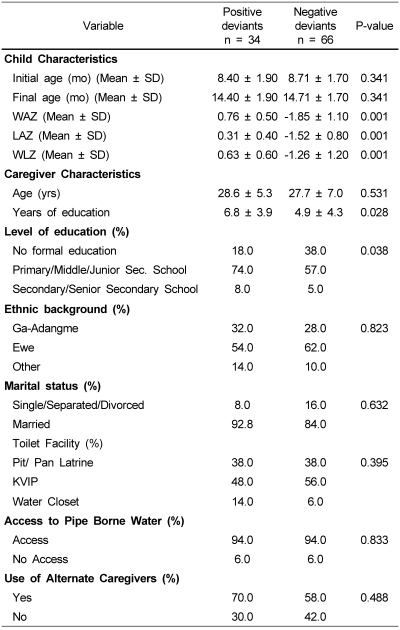
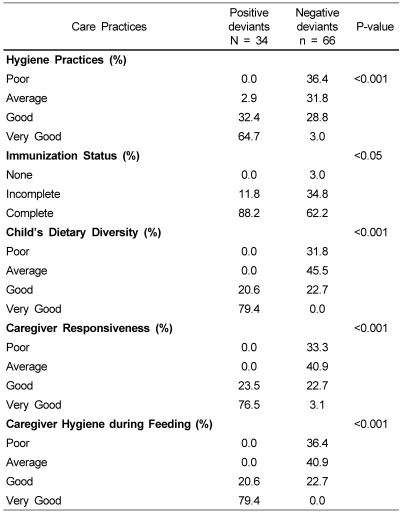
The background characteristics of caregivers and the children are presented in Table 1. Apart from education, background characteristics of caregivers of positive and negative deviants were comparable in most aspect. Caregivers of positive deviant children were more educated. About a third of the caregivers of negative deviant children had no formal education. The mean WAZ, LAZ and WLZ of the negative deviants were significantly lower (p ≤ 0.05) than that of the positive deviants. Table 2 shows care practices in relation to child nutritional status. A significant difference was observed between caregiver hygiene practices and child nutrition deviance status. Caregivers of positive deviant children practiced better hygiene and were more likely to keep themselves, children and their surroundings clean. This was evidenced by 97.1% caregivers of positive deviants being categorized as exhibiting 'good to very good hygiene practices' as compared to 31.8% of caregivers of negative deviant children. Although immunization coverage was high between the two groups, the overall mean score was significantly higher among the positive deviant children. By the end of the observational study, the majority of the positive deviants had fully completed their immunization schedules. On the contrary, 3% of the negative deviants had not received any immunization at all, with a third yet to complete their immunization.
Dietary diversity scores for the two groups were significantly different, with positive deviant children having more diversity in their diet. The majority of the positive deviant children were rated 'very good' in dietary diversity. None fell within the 'average' or 'poor' dietary diversity category. This indicates that positive deviant mothers fed their infants and young children a variety of food items from the different food groups. On the contrary, most of the negative deviants had dietary diversity ratings that were in the poor to average category. Only 23% fell within the 'good' dietary diversity grouping.
Caregiver ability to feed responsively also differed significantly between the two groups. Caregivers of positive deviants were highly responsive during feeding. They were more likely to demonstrate eating, supervise feeding, encourage the child, offer more food and less likely to threaten or order the child to eat. This is evidenced in a 100% 'good to very good' responsive behaviour rating exhibited by these caregivers. In terms of hygiene practices related to feeding, significant differences were observed between the two groups of caregivers, with caregivers of positive deviants exhibiting better hygiene practices. They were more likely to wash their hands before and after feeding, use clean water and soap to wash hands, dry hands with clean towels and feed with clean utensils as well as keep a cleaner feeding environment. Seventy nine percent (79%) of caregivers of positive deviants showed 'very good' hygiene practices as against 23% of the negative deviants, with as many as a third of caregivers of negative deviants exhibiting poor hygiene practices.
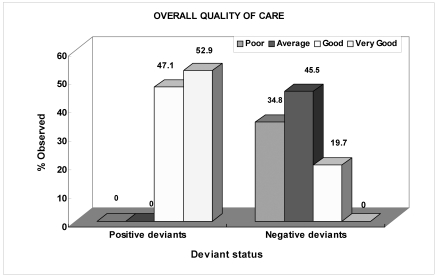
Fig. 1 shows that the overall quality of child-care practice score was better among caregivers of positive deviants than negative deviants. For positive deviant caregivers, the overall quality of care was between good and very good. On the contrary, only a fifth of caregivers of negative deviants were rated as exhibiting "good" quality of care practice; with the rest being rated as showing "poor to average" quality of care. Caregivers of positive deviants were more likely to practice good household and personal hygiene, complete their children's immunization schedules, provide complementary foods from diversified sources, exhibit high responsiveness during feeding, and also feed under hygienic and cordial environment.
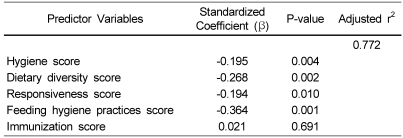
An analysis to determine how the various care indicators predicted a child's nutrition deviance status and hence nutritional status using the regression model revealed that although overall immunization status was significantly different between the two groups, it lost its significance when the other variables were controlled for (Table 3). The remaining variables were all negatively associated with child nutrition deviance status.
Discussion
The objective of this study was to assess how caregiving practices influence nutritional status of young children in Ghana. The major findings are discussed in this section.
The importance of parental education for the health and well being of the child has been stressed by many (Amar-Klemesu et al., 2000; Guldan et al., 1992; Vella et al., 1992). Positive associations between maternal educational level and children's health and nutritional status have been reported by Vella, et al. (1992). Parental education could function by lowering fatalistic attitudes to illness, increased belief in the possibility of changing children's health status, acceptance of new ideas, greater confidence in dealing with health professionals and taking more direct responsibility for child rearing practices. In Bangladesh, Guldan et al. (1992) reported a close association between maternal education and child nutrition. Educated mothers gave their children complementary foods more frequently, fed in a more protected and cleaner settings and had healthier babies. Among Ghanaian mothers, various studies have identified maternal education as a crucial asset for good caregiving practices and an important determinant of child growth in the first 18 mo of life (Amar-Klemesu et al., 2000; Lartey et al., 2000). Similar studies elsewhere have also reported positive associations between maternal education, child health and nutrition (Cebu Study Team, 1991; Le Vine et al., 1991; Tucker & Sanjur, 1988). In the present study, the highly positive caregiving behaviors among the positive deviant mothers could be explained by their higher educational status. Interventions to promote girls/women's education would thus go a long way to improve care practices and child nutrition in this population.
Personal and household hygiene practices are critical for positive health and nutrition outcomes. The poor hygiene and sanitation conditions prevailing among the negative deviant group can impact negatively on their health status. Good caregiver hygiene practices such as cleanliness of the child, mother and surroundings, have been reported to be significantly correlated to child nutritional status and morbidity (Amar-Klemesu et al., 2000; Zeitlin, 1994). In Bangladesh, ground cleanliness was reported to be strongly associated with child morbidity especially during ages when children were crawling (Ahmed et al., 1993). Bartlett et al. (1992) reported significant associations between mother's dirty hands and faeces on the ground with persistent diarrhoea among children. In Nicaragua, Gorter et al. (1998) reported significant associations between hygiene indicators and diarrhoea. Interventions to improve hygiene and sanitation in poor communities will help improve child health and nutrition.
Dietary diversity, the number of different foods or food groups consumed by an individual, provides a measure of the quality of the diet and it is particularly important for micronutrient status. With the exception of breastmilk, nutrients essential to meet the nutritional requirements of an individual are not found in a single food item but come from a diet composed of a variety of foods. Diverse diets have been shown to protect against chronic diseases such as cancer (Vecchia et al., 1997) as well as being associated with improved health, nutrition and longevity of life (Ferguson & Opare-Obisaw, 1993; Hodgson et al., 1994; Kant et al., 1995). Several dietary guidelines have emphasized the importance of eating a variety of foods (Chinese Nutrition Society, 1990; Drewnoswski et al., 1997). Dietary diversity has been reported to be associated with child nutritional (Arimond & Ruel, 2004). The low diet diversity scores among the negative deviant children could increase their risk of micronutrient deficiencies.
Caregiver responsiveness during feeding is also particularly important to child health and nutrition outcomes. The findings of the present study revealed more active care giving among caregivers of positive deviant children. Several studies have reported significant associations between caregiver's active role in child feeding and child nutritional status (Dettwyler, 1986; Engel & Zeitlin, 1996; Zeitlin et al., 1989). In Mexico, Zeitlin et al. (1989) reported significant associations between feeding activity and child's height-for-age among children between the ages of 8 to 22 months. More active feeding behaviors were associated with increased dietary intake and greater anthropometric scores. Dettwyler (1986) also observed positive caregiver attitude as a predictor to child weight-for-age than socio-economic status in Mali. Poor growth was reported to be associated with a lack of parental supervision of meals, irregular meal times and parental indifference among 136 children aged 4 to 36 months. Interventions that use behavior modification strategies may help improve child-caregiver interactions during feeding and bring about changes in feeding behaviours.
The marked difference in hygienic practices during feeding between the two groups of caregivers is quite surprising considering the fact that they have similar cultural background. The higher level of education of positive deviant caregivers may account for this difference. Good hygiene practices during feeding contribute to positive health and nutritional outcomes. Intensifying education on good hygiene and sanitation during feeding will help enhance good nutrition and health among young people in this community.
The quality of care provided by a caregiver has a significant effect on nutrition deviance status of children. Although the quality of care provided by a caregiver has been conceptualized to have significant effect on child nutritional outcome, only one study has actually assessed the quality of caregiving and child nutritional status in Ghana. In their study of care practices in Accra, Ruel et al. (1999) reported a strong association between caregiver quality of care practice and child nutritional status in terms of weight-for-age and height-for-age. The findings of the observational study corroborated that childcare was one of the important discriminating factors between positive and negative deviant children. The results of our study revealed that, in this population, quality of care practices are significantly associated with child nutrition and the child's nutrition deviance status. Caregivers who exhibited better quality of care practice produced positive deviant children in the community. Thus care practices on nutritional status as reported by Ruel et al. (1999) among urban poor in Accra is similar to that observed among the rural poor in Manya Krobo. There was however a loss of association between immunization and child nutritional status when the effects of the other four care variables were taken into consideration. This suggests that for this sample, immunization primarily affected child nutritional status through its association with good hygiene, good dietary diversity, high responsiveness and good hygienic practices during feeding.
The findings of this study have confirmed the notion that better caregiving promotes growth and nutrition among young children. Caregiving behaviours that contribute to good nutritional status of children include among others, good young child complementary feeding practices, immunization, and good hygiene and sanitation. Promoting the practice of these behaviours could lead to improved child health and nutrition. The development of mother support groups in communities could be a good strategy to provide emotional help to mothers, with mothers of positive deviant children being used as role models to transfer and share their maternal practices with mothers of poor growing children.
 XML Download
XML Download