

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
The incidence of diabetes among the Korean population has continuously increased in the recent twenty years (Kim et al, 1998). Thus, the high prevalence and death rate from diabetes in Korea now places the country in the highest quartile group among the OECD countries (Ministry of Health & Welfare, 2007). The National Health and Nutrition Examination Survey for Koreans conducted in 2005 showed that the prevalence of diabetes was 9.0% for males and 7.2% for female adults (Ministry of Health & Welfare 2006).
Type 2 diabetic patients are characterized by reduced secretion of insulin and increased insulin resistance, resulting in elevated blood glucose levels (Salgueiro et al., 2001). Zinc is known to be an essential micronutrient involved in the physiological action of insulin (Roth & Kirchgessner, 1981). Animal studies suggested that glucose tolerance in conjunction with insulin resistance aggravated after zinc deprivation (Kinlaw et al., 1992; Salgueiro et al., 2001). However, the relationship of zinc deficiency and glycemic control in diabetic patients has not been well established. Inadequate zinc intake induces higher absorption throughout the intestine resulting in less urinary excretion by homeostatic compensation mechanism in healthy subjects. Meanwhile, increased urinary excretion of zinc has been observed in several studies (Chausmer 1998; Cunningham et al., 1994; Salgueiro et al., 2001).
Previous studies indicated that the zinc status of Korean diabetic patients is at the marginal level (Lee et al., 2005; Yoon & Lee, 2007). Zinc intake has a positive relationship with the protein and fat intake, but is negatively correlated with the carbohydrate intake. Foods with high amounts of phytate were the major source of zinc, and therefore, did not contribute to increasing zinc densities of frequently consumed foods (Yoon & Lee, 2007).
It is known that regular physical activity lowers the risk of type 2 diabetes mellitus by 20-60% in dose-related manner. The size of the effect is greatest in subjects with high risk of non-insulin dependent diabetes (Vuori, 2001). Therefore, maintaining a moderate physical activity pattern along with dietary management is regarded as an essential element for glycemic control and weight reduction of diabetic patients. However, it is not yet explicated whether physical activity level is related to improving zinc status as well. Therefore, in this study, we assessed the quality of diet, glycemic control, and zinc status of diabetic patients and normal adults by using self-reported physical activity levels to figure out the association among physical activity level, glycemic control, and zinc nutrition. In particular, we aimed to explicate whether the diabetic patients with proper physical activity levels could also maintain better dietary practices, thereby improving their zinc status.
Subjects and Methods
Selection of subjects
Among adults visiting community public health centers or local clinics in the Daegu area, seventy-six type 2 diabetic patients with no known medical problems voluntarily participated in this study. In order to collect general characteristics such as age, education, physical activity level, medication, diabetic duration and complication, patients were interviewed by a trained dietitian.
Anthropometric assessment
While the subjects were wearing light indoor clothes and no shoes, body weight was measured to the nearest 0.1 kg, and height was measured to the nearest 0.5 cm. Circumferences of waist and hip were measured to the nearest 0.1 cm. Body mass index (BMI) was calculated from measured height and weight for each subject. Body fat content and percentage body fat were assessed using the Bio-electrical Impedance Fatness Analyzer (GIF-891).
Assessment of dietary intake
Information on the dietary intake of each subject was collected for two non-consecutive days during the week by the 24-hour dietary recall method. Food pictures were provided for the subjects to improve the accuracy of estimation of actual intake (Korean Food Research Institute, 1998).
Food intakes were converted to the amount of daily nutrients intake by CAN-Pro 3.0 (developed by Korean Nutrition Society). Dietary inadequacy of each nutrient was estimated from the proportion of subjects with intakes below the Estimated Average Requirement (EAR). Dietary diversity score (DDS) was assessed by the six-food group system described in the Dietary Reference Intakes for Koreans (KDRIs) (Korean Nutrition Society, 2005). Dietary variety score (DVS) was calculated as the average total number of food items consumed in a day by each subject from the 24-hour recall data.
Measurement of physical activity level
Three levels of physical activity (i.e. light, moderate, and heavy) were constructed as follows. Participants with a sedentary life style were classified into the "light physical activity" group. Those who walk or cycle regularly more than once a week were placed in the "moderate physical activity" group. Subjects engaging in regular exercise such as jogging or swimming at least 4-5 times a week were sorted into the "heavy physical activity" group. After explaining the typical activity patterns representing light, moderate, heavy physical activities, each subject was asked to rate his or her physical activity level into one of the three levels: light, moderate or heavy.
Biochemical assessment
As for biochemical markers of individual zinc status, we measured the zinc levels in serum and urine. A fasting blood of 10 ml was collected from each subject and prepared serum samples were stored at -70℃. Serum glucose levels and HbA1c were measured for the assessment of blood glucose control. Urine samples for 24 hours were collected for one day from each subject. Urinary creatinine was measured using Hawk's method (Hawk, 1954). Urinary zinc was analyzed by Inductively Coupled Plasma Emission Spectroscopy (ICP) (Jobin Yvon, 38 plus, France). Serum level of zinc was assessed by atomic absorption spectrometry.
Statistical analysis
The Statistical Analysis System (SAS) Package was used to analyze the relationship among glycemic control status, dietary factors, and physical activity levels. Data were presented as mean ± SD. The statistical significance of differences in dietary quality, zinc status, and glycemic control among different physical activity level groups was tested by using one-way analysis of variance (ANOVA) and Duncan's multiple range test.
Results
Subject characteristics
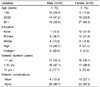
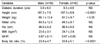
The general characteristics of the subjects are described in Table 1. The age distribution indicated that female diabetic patients who participated in this study were older than their male counterparts. As indicated in Table 2, there were no significant differences in body mass index (BMI), waist circumference, hip circumference, and waist-hip ratio (WHR) between males and females. Diabetic duration was 5.0 ± 6.2 years for men, 6.5 ± 4.6 for women.
Dietary quality and nutrient intake
Table 3 shows the profile of nutrition inadequacy estimated by the percentage of subjects whose nutrients intake was less than the EAR. More than half of the subjects showed dietary inadequacy for five nutrients such as riboflavin (= 82.9%), calcium (= 76.3%), thiamin (= 63.2%), zinc (= 56.6%) and vitamin C (=52.6%).
The average daily intake of each food group classified by KDRIs is presented in Table 4. Dietary intakes from the meat, poultry, fish, egg and bean (MPFEB) food groups and the milk food group were lower than the recommended level suggested for 1800 kcal of energy intake level.
Zinc status, glycemic control and dietary quality by physical activity level
Results for dietary zinc intakes, as indicated in Table 5, show that zinc intake of the participants was not significantly different across groups classified by self-reported physical activity levels. However, we observed a tendency for higher zinc intake among those who reported "heavy" level of physical activity. Serum zinc level of diabetic patients was significantly lower for the "light" physical activity group, whereas no significant difference was found in urinary zinc excretion.
Table 6 compares the results of HbA1c and fasting blood glucose, which are possible indicators of glycemic control, by the physical activity level. Both fasting blood glucose and HbA1c were slightly higher in the "light" physical activity group, compared to those in the "moderate" or "heavy" physical activity group. However, these differences were not significant.
Table 7 shows the DDS and the DVS of the participants by physical activity levels. While the DDS was not significantly different across physical activity levels, the DVS was significantly lower among those engaging in light physical activities.
Discussion
In this study, we compared the zinc status, glycemic control indices, and the dietary quality of diabetic patients by their self-reported level of physical activity.
In general, diabetic patients showed a poorer intake of nutrients than the average Korean adult reported by National Health and Nutrition Examination Survey in 2005. In particular, a higher prevalence of riboflavin and calcium inadequacy was observed for diabetic patients and analyzed by the percentage of subjects with dietary intakes less than the EAR. This is possibly attributable to the insufficient consumption of milk. Out data demonstrated that the dietary intake of the meat, poultry, fish, egg, and bean food groups, and the milk food group, was lower than the daily-recommended level of 1800 kcal (Korean Nutrition Society, 2005).
There seems to be no general consensus on the protein intake for diabetes. Eating less protein has been recommended to avoid accelerating renal complications. Human trials, in which meat was withdrawn from the diet, have been reported to successfully reduce albuminuria in type 2 diabetes with macroalbuminuria (de Mello et al., 2006). However, other investigators suggested that there is no reason to restrict protein in diabetes without clear renal indications to do so (American Dietetic Association, 2002; Eckel, 2006). Considering the fact that the bioavailability of zinc from animal sources is higher than from grain or vegetables, less intake from the animal food group could lead to inadequate zinc status in diabetic patients. Concerns on marginal zinc deficiency have also been reported by other investigators (Chausmer 1998; Kwun & Kwon, 2000; Lee et al., 2005; Lonnerdal, 2000; Salgueiro et al., 2001).
Most strategies of diabetes management encourage physical activity as well as healthy food choice to improve blood glucose control and weight loss for type 2 diabetes as increased physical activity can lead to improved glycemia and decreased insulin resistance (American Dietetic Association, 2002; Vuori, 2001). However, we did not find any statistically significant difference of glycemic control indicators across different physical activity levels. A decrease in blood glucose levels and HbA1c along with higher level of physical activity was observed in diabetic patients. Since the physical activity level was solely based on self-rating without any objective measurement for the detailed activity pattern of each subject, the classification of activity levels was not accurate enough to detect small differences in indicators across groups. It has been already known that diabetic patients benefit from regular physical activity in many ways such as increased insulin sensitivity, decreased need for insulin, and lower blood peak glucose levels (Vuori, 2001; Wallenberg-Henriksson et al., 1998).
For the evaluation of dietary quality, the dietary variety score is generally accepted as one of the convenient measures (Choi et al., 2000; Drewnoski et al., 1998; Kant, 1996), since consumption of different food items is expected to improve the overall quality of diet and the nutritional status. Our study showed that maintaining physical activity above moderate levels contributes to consumption of more diverse food items. It seems that the diabetic patients with proper physical activity levels would pay more attention to health and pursue health-promoting behaviors including dietary practices.
Our findings of higher urinary zinc excretion in diabetic patients are consistent with the previous studies (Cunningham et al., 1994; Lee et al., 2005; Pidduck et al., 1970). A recent study also showed higher urinary levels of trace elements in diabetic patients compared to their age-matched healthy controls (p<0.001). They reported that mean values of zinc levels in blood was reduced in diabetic patients compared with control subjects. However, these differences were not significant (Kazi et al., 2008).
Although it has been speculated that the continued zinc loss through urinary excretion may result in zinc deficiency in diabetes, the correlation between urinary zinc and serum levels of zinc was not well demonstrated in previous studies (Levine et al., 1983; Mateo et al., 1978; Mooradian & Morley, 1987). In this study, higher serum zinc levels were shown in diabetic patients with heavy physical activities. It is beyond the scope of this study to draw any definite conclusions on the relationship between physical activity and zinc status. However, we believe that physical activity may potentially contribute to improving zinc status by improving the overall dietary status.
In conclusion, our study indicated that poorer dietary quality and zinc status were observed in diabetic patients with less physical activity. Therefore, more attention is needed to improve the zinc status among Korean diabetic patients, whose activity patterns tend to be sedentary. Appropriate nutrition education is urgently required for diabetic patients as well as the general adult population to attain dietary adequacy and to increase the amount of their physical activities.





 XML Download
XML Download