

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
The prevalence of diabetes mellitus has been rapidly increasing in Korea. Diet plays a key role in the treatment of diabetes and proper nutrition is vital to prevent diabetes complications (Park & Ahn, 2007). However, it is not an easy task to follow diabetic diet prescription and the compliance with diabetic diet recommendations is reported to be very poor (Woo et al., 2006). In recent years, functional foods have appeared as new means to help maintain proper nutrition in patients with chronic diseases such as diabetes.
Spirulina (arthrospira platensis) has received much attention as functional food regarding its association with cholesterol-regulatory properties, modulation of the host immune system, and antioxidant capacity (Hirata et al., 2000; Qureshi et al., 1995). There is increasing scientific and clinical evidences for its role in controlling chronic diseases such as diabetes (Iyer et al., 2001), arthritis (Mishra et al., 1998), anemia (Iyer et al., 2000) and cancer (Mathew et al., 1995).
Spirulina is a microscopic and filamentous cyanobacterium (blue-green alga) that has a long history of use as a food for humans. Spirulina is a rich source of protein and vitamins, especially vitamin B12, minerals, carotenoids, and phycocyanins. Its safety as food has been established through toxicological study (Salazar et al., 1996).
We have also reported that spirulina supplementation to healthy elderly people resulted in significant reductions of plasma triglycerides, total-and LDL-cholesterol, blood pressure, and improving the antioxidant status, as well as inflammatory status and came to conclusion that it was suitable as a functional food for elderly people (Park & Kim, 2003; Park et al., 2008). However, the effect of spirulina as a functional food for patients with diabetes has not been evaluated. In this study, we aimed to evaluate the effectiveness of spirulina as functional food in Korean patients with type 2 diabetes.
Subjects and Methods
Subjects and experimental protocol
The study subjects were recruited from a diabetes clinic in Seoul from September 2007 to May 2008. Current users of medications for diabetes, dyslipidemia, and inflammatory diseases and of vitamin supplements were excluded. Finally 37 subjects (20 male, 17 female) were enrolled in this study. The research protocol was approved by 'Institutional Review Board (IRB)' of Yonsei University. All subjects gave written informed consent before beginning the study.
At the first visit for intervention study, blood was drawn after a minimum of 12 h of fasting. Anthropometric and biochemical parameters and nutrient intakes were measured for baseline data. The enrolled subjects were randomly assigned into either spirulina or control group. When the subject entered the trial, the subject chose a numbered sealed envelope containing the randomized allocation to the spirulina (intervention) or control (no intervention) group.
The subjects in spirulina group received 40 pills containing 0.2 g of freeze-dried spirulina (8.0 g/day) for 12 consecutive weeks and control group was instructed not to take any functional foods or supplements. During the intervention period, both spirulina and control groups were asked to maintain their usual diets and levels of physical activity. They were also required to abstain from taking any other supplements.
The compliance for all subjects was confirmed by telephone twice a week. Anthropometric and biochemical parameters were measured before and after the intervention period for both spirulina and control groups. The spirulina was provided by Earth Spirulina Group (ES Co, Seoul, Korea) and sent to subjects every 2 weeks.
Anthropometric, hematological and dietary assessment
The subjects were individually interviewed to obtain general characteristics, life-style behavior and food consumption. Body weight, height and body composition were measured using In-body 4.0 (Biospace Co. Korea) and body mass index (BMI, kg/m2) was calculated. Waist circumference was measured by a tapeline and abdominal fat thickness was assessed by ultrasonographic measurement (General Electric logic 7. USA). The systolic and diastolic blood pressures were measured twice using an automatic blood pressure calculator (Biospace Co. Korea) after 10 minute rest.
The daily nutrient intakes were assessed using Food Frequency Questionnaire (FFQ). Dietary intakes data were analyzed by Can-pro 2.0 software (The Korean Nutrition Society, Korea).
Serum levels of glucose, triglyceride, total-cholesterol, and HDL-cholesterol were measured using an autoanalyzer (COBAS MIRA. Roche. Switzerland). LDL-cholesterol and atherogenic index (AI) were calculated as described by Friendewald et al. (1972) and Lauer et al., (1998), respectively [LDL-cholesterol=Total cholesterol-HDL-cholesterol-(Triglyceride / 5), Atherogenic index (AI)=(Total cholesterol-HDL-cholesterol / HDL-cholesterol)]. The analysis of insulin was performed at 'Seoul Medical Science Institute (SCL)' and Hemoglobin A1c was measured using an analyzer (HLC-723 G7, Tosoh, Japan).
The KITT value (%/min, insulin tolerance test) was used to assess insulin resistance. Insulin (Humulin®, RI 0.11 U/kg body weight) was given intravenously after a 12 h fast. Plasma glucose was then measured at 0, 3, 6, 9, 12, and 15 min. After the plasma glucose levels were converted to natural logarithms, the slope of the reduction in plasma glucose (KITT) was calculated: KITT = 0.693/t1/2×100 (%/min) (Monzillo & Hamdy, 2003).
Inflammation and antioxidant status assessment
Serum adiponectin concentration was determined with enzyme linked immunosorbent assay (ELlSA) kits (Mesdia Technology Inc., Korea) according to the manufacturer's instructions. Ten microliters of serum samples were assayed in parallel to known adiponectin recombinant concentrations. Each assay was calibrated using an adiponectin standard curve.
Serum IL-6 and TNF-α concentrations were determined by enzyme linked immunosorbent assay (ELlSA) technique (Quantikine, R&D Systems Inc., USA) reading ELISA reader (Spectra Max 340, USA).
Serum malondialdehyde (MDA) level, an index of antioxidant capacity, was measured using a Lipid Peroxidation Assay kit (Oxford Biomedical Research, USA). This assay is based on the reaction of a chromogenic reagent, N-methyl-2-phenylindole (R1), with MDA at 45℃. The reactive product produces a chromopore that has a stable violet color, the intensity of which is measured at 586 nm. MDA concentration was calculated using a MDA standard curve.
Statistical analysis
Statistical analysis was performed with the SPSS program (version 12.0). Data were presented as mean ± S.E. Chi-square test was performed to determine differences at baseline in frequencies of categorized variables between the groups and mean differences were analyzed by analysis of covariance (ANCOVA). Paired t-test was used to analyze mean differences for all measured parameters between baseline and end of intervention period. To demonstrate the association between baseline blood profiles and mean change of various parameters, partial correlation coefficients analysis was conducted. Data within each group were analyzed by repeated measures analysis of variance to establish significant differences in treatment. The P value of less than 0.05 was considered statistically significant.
Results
There were no significant differences in baseline characteristics between spirulina and control groups such as age, sex and diabetic family history, cigarette smoking, alcohol consumption (Table 1). Also, no differences were found in anthropometric and hematological parameters and dietary intakes.
Blood profiles during the intervention period
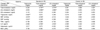
After 12 weeks of intervention, no significant changes were observed in the plasma levels of fasting blood glucose (FBG), hemoglobin A1c, insulin, total cholesterol, LDL-cholesterol, and HDL-cholesterol in either group (Table 2). The atherogenic index, KITT, and blood pressure also were not significantly changed for both spirulina and control groups. However, plasma level of triglycerides was significantly decreased (from 125.8 mg/dl to 98.5 mg/dl, p<0.05) after the spirulina intervention. Spirulina supplementation showed a significant lowering effect on plasma triglyceride level and diastolic blood pressure by repeated test for treatment (time × treatment interaction, p<0.05).
Inflammation and antioxidant status during the Intervention period
Changes of plasma levels of inflammatory cytokines and MDA during 12 weeks of intervention period are shown in Table 3. In spirulina group, the plasma level of malondialdehyde (MDA) was significantly decreased (from 2.57 µM/L to 1.85 µM/L, p<0.01) and the plasma level of adiponectin showed a tendency of an increase (from 5.52 µg/ml to 6.62 µg/ml, p<0.1). No differences were observed in the concentrations of TNF-α and IL-6 between baseline and end of 12-week intervention period. On the other hand, the plasma levels of MDA, adiponectin, TNF-α, and IL-6 were not changed after 12 weeks of intervention in control group. Repeated test for treatment showed significant effects of spirulina supplementation on lowering plasma MDA (time × treatment interaction, p<0.05) and on increasing adiponectin concentration (time × treatment interaction, p<0.05).
Effect of intervention according to blood lipids level at baseline
The effect of spirulina supplementation may differ whether the subjects have dyslipidemia or not before entering intervention study. Therefore, we assessed the correlations between baseline blood lipids level and changes of biochemical variables in spirulina supplemented subjects (Table 4).
The plasma level of triglyceride at baseline was negatively correlated with changes of triglyceride (r=-0.605, p<0.01) and systolic blood pressure (r=-0.538, p<0.05). Also, plasma level of total cholesterol at baseline was negatively correlated with changes of plasma concentrations of total cholesterol (r=-0.787, p<0.01), LDL-cholesterol (r=-0.665, p<0.01), and IL-6 (r=-0.552, p<0.05), and systolic (r=-0.527, p<0.05) and diastolic blood pressure (r=-0.600, p<0.01). Plasma level of LDL-cholesterol at baseline showed significant negative correlations with changes of total cholesterol (r=-0.734, p<0.01), LDL-cholesterol (r=-0.689, p<0.01), diastolic blood pressure (r=-0.516, p<0.05) and IL-6 (r=-0.532, p<0.05). On the other hand, these trends were not found in control subjects. This result indicates that subjects with higher lipid concentrations before entering intervention study showed higher reduction in lipids, inflammatory cytokine levels, and blood pressure by spirulina supplementation. However, changes in insulin resistance, adiponectin concentration and antioxidant capacity were not affected by initial blood lipid levels of the subjects.
Discussion
Spirulina is reported to be effective for improving blood lipid profiles (Torres et al., 1998), enhancing immune capacity, and reducing oxidative stress (Shklar & Schwartz, 1998). Since dyslipidemia, oxidative and inflammatory stress are considered to be the contributing factors for diabetes, spirulina is the most likely candidate as functional food for management of type 2 diabetes.
Park (2007) reported that spirulina supplementation to healthy elderly people with normal fasting blood glucose (FBG) brought a significant reduction in mean FBG from 105.1 mg/dl to 100.0 mg/dl. On the contrary, the spirulina supplementation in patients with type 2 diabetes in this study did not result in a reduction in the plasma levels of FBG, hemoglobin A1c, and insulin. The subjects in this study were type 2 diabetes mellitus (DM) patients with FBG>126 mg/dl. Therefore spirulina may not have beneficial effect on blood glucose concentration for DM patients.
Many animal and human studies have repeatedly reported the lipid-lowering effects of spirulina. Park and Kim (2003) reported that the plasma levels of triglyceride, total cholesterol, and LDL-cholesterol in Korean elderly people were significantly decreased after spirulina supplementation for 24 weeks. Also, spirulina supplementation to type 2 diabetic patients resulted in a significant decrease in plasma concentrations of triglyceride, total cholesterol and LDL-cholesterol (Iyer et al., 2001). In an animal study, rats fed a 20% water-soluble fraction of spirulina showed a significant reduction in LDL/HDL ratio (Hosoyamada et al., 1991). In our study, no changes were observed in plasma concentrations of total cholesterol, LDL-cholesterol, and HDL-cholesterol after spirulina intervention, however, a significant lowering effect on plasma triglyceride concentration was shown. The less profound cholesterol lowering effect in this study may be due to baseline lipid concentration of the subjects. The cholesterol concentrations of our subjects at baseline were in normal ranges, however, the baseline lipid profile of the previous study (Park & Kim, 2003) was higher with triglyceride of 168.2 mg/dl, and total cholesterol of 231.3 mg/dl, and LDL-cholesterol of 154.6 mg/dl. Correlation analysis in this study revealed that subjects with higher initial blood levels of triglycerides and cholesterol showed a higher reduction in lipid concentration, blood pressure and inflammatory cytokine. Therefore, spirulina supplementation was probably more effective for lowering total cholesterol in subjects with higher blood cholesterol level before intervention.
Hypotriglyceridemic and blood pressure lowering effects of spirulina have been reported. Iwata et al. (1990) postulated that the hypotriglyceridemic effect of spirulina might be due to its effect on the metabolism of lipoproteins. They reported that rats fed a diet containing spirulina showed a significant increase in the activity of lipoprotein lipase compared to rats fed a high fructose diet. The mechanisms of spirulina on blood pressure are not well understood. However, Guan et al. (2007) have proposed that the high potassium content of spirulina may have a lowering effect on blood pressure.
Oxidative stress may play an important role in the etiology of diabetic complications (Giugliano et al., 1996). Kim and Kim (2005) reported that healthy elderly subjects received spirulina supplementation for 8 weeks showed improved antioxidant status as evidenced by increased total antioxidant status and decreased thiobarbituric acid reactive substance. In accordance with these studies, spirulina supplementation in this study resulted in a significant decrease in MDA level from 2.57 µM/L to 1.85 µM/L. Also, a significant increase in plasma adiponectin concentration was observed in this study after spirulina supplementation. An increase in adpionectin concentration with a decrease in oxidative stress would play a role in the prevention of DM complication.
In conclusion, spirulina intervention brought in favorable effect on blood lipids, anti-oxidant capacity, and inflammatory response in Korean patients with type 2 diabetes. Our results also suggest that spirulina is a promising agent as a functional food for the management of diabetes. Further studies with larger sample size and longer duration are required to ascertain the mechanism of spirulina's actions on lipid profiles, immune variables, and antioxidant capacity.



 XML Download
XML Download