

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Obesity is one of the most common disorders in clinical practice and closely associated with a number of pathological diseases, such as non-insulin-dependent diabetes, hypertension, and atherosclerosis (Gregoire et al., 1998). Although rare, obesity can be caused by mutations in a single gene. However, the greatest proportion of obesity involves the interaction variants in multiple genes with environmental factors, particularly diet (Loos & Bouchard, 2003; Loss & Rankinen, 2005). In addition, several lines of studies suggested a close association between insulin signaling and obesity. Kadowaki et al. (2003) have reported the molecular mechanisms of insulin resistance and obesity, focusing on the function of adipocyte.
Pre-B-cell leukemia transcription factor (PBX1) is a member of a ubiquitous class of homeodomain proteins. The PBX1 gene, localized on chromosome 1q23, was originally identified by its involvement in a t (1;19) chromosomal translocation in acute pre-B-cell leukemias (Kamps, 1990; Nourse et al., 1990). Subsequent study has shown that PBX1 is widely expressed and acts as a cofactor for a variety of HOX proteins (Sagerstrom, 2004). These homeodomain transcription factors in turn regulate developmental gene expression and early embryonic development and organogenesis, and maintain differentiated cell states (Sagerstrom, 2004).
The role of PBX1 has been well studied in the pancreas, where it complexes with and regulates the key β-cell homeobox protein, PDX1 (IPF1 in humans) (Wang et al., 2005). In mice, PDX1 activity was sufficient for the development of the major cell types, but PBX1:PDX1 complex was essential for the expansion of each cell type within the developing pancreas, and hence for normal pancreatic development (Dutta et al., 2001). Dutta et al. (2001) also suggested that PBX1:PDX1 heterodimer contributes to ductal cell proliferation and subsequent islet regeneration. Kim et al. (2002) examined pancreatic Pbx1 expression, morphogenesis, cell differentiation, and function in mice deficient for Pbx1. Pbx1 -/- embryos had pancreatic hypoplasia and marked defects in exocrine and endocrine cell differentiation prior to death at embryonic day 15 or 16. Pbx1 +/- adults had pancreatic islet malformations, impaired glucose tolerance, and hypoinsulinemia. Consequently, Kim et al. (2002) concluded that PBX1 is essential for normal pancreatic development and function and perturbation of PBX1 activity may also promote susceptibility to diabetes mellitus.
Despite potentially important roles in metabolic diseases, genetic association of PBX1 on obesity is not yet unknown in humans. Therefore, we examined whether PBX1 polymorphism contributes to the susceptibility to obesity or obesity-related metabolism traits in a Korean population.
Materials and methods
Study subjects
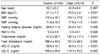
The body mass index (BMI) was calculated from height and weight using the formula: BMI=body weight/(height)2 in kg/m2. In the World Health Organization guidelines for Asians, individuals with a BMI≥23 kg/m2 are classified as overweight and those with a BMI≥25 kg/m2 are defined as obese (World Health Organization Expert Consultation, 2004). We recruited a case group (n=214) that comprised overweight and obese subjects (BMI≥23 kg/m2, 123 men and 91 women) and control subjects (n=160) with normal weight (BMI: 18.0-22.9 kg/m2, 66 men and 94 women) at Kyung Hee University Medical Center and Keimyung University Dongsan Medical Center. All of the subjects were ethnic Koreans. Blood samples were drawn for biochemical measurements, i.e., fasting plasma glucose, hemoglobin A1c (HbA1c), triglyceride (TG), total cholesterol, high-density lipoprotein cholesterol (HDL-C), and low-density lipoprotein cholesterol (LDL-C). The clinical characteristics of the subjects were summarized (Table 1). DNA was isolated from peripheral blood leukocytes using the G-DEX™ IIb Genomic DNA Extraction Kit (iNtRON Biotechnology, Seongnam, Korea). All of the subjects gave written informed consent before entering the study. This study was approved by the Institutional Review Board of Kyung Hee University Medical Center.
Determination of genotype
Initially, we selected 66 single nucleotide polymorphisms (SNPs) within the PBX1 gene using the following criteria: (1) consisting only of SNPs in introns (approximately 300bp from the exon to consider alternative splicing); (2) tagging SNPs selected using the tagging option of the program Tagger (http://www.broad.mit.edu/mpg/tagger/); (3) known heterozygosity and minor allele frequency (MAF) > 0.05; and (4) reported validation (http://www.hapmap.org). The genotyping was performed using the Affymetrix Targeted Genotyping Chip array (Affymetrix, CA, USA), according to the manufacturer's protocol. This chip uses molecular inversion probe technology with gene chip universal microarrays to provide a method that is capable of analyzing thousands of variants in a single reaction. In brief, DNA was digested and then subjected to PCR using primers specific to the adaptor sequence. PCR products were purified and the fragmented DNA was then end-labeled with biotin using terminal deoxynucleotidyl transferase. Labeled DNA was then hybridized onto the Mapping Array. The hybridized array was washed, stained, and scanned according to the manufacturer's instructions. The image was analyzed using GCOS software (Affymetrix).
Statistical analysis
For the case-control association study, Hardy-Weinberg equilibrium (HWE) for all SNPs was assessed using SNPstats. (Solé et al., 2006) A linkage disequilibrium (LD) block of polymorphisms was tested using Haploview (version 3.32) (MA, USA). (Barrett et al., 2005) Multiple logistic regression models were calculated for the odds ratio (OR), 95% confidence interval (CI) and corresponding P values, controlling for age and gender as covariables. We used SNPstats, HapAnalyzer version 1.0 (Seoul, Korea) (Park et al., 2008) and SNPanalyzer (ISTECH Inc., Goyang, Korea). The power of the sample size was calculated using a genetic power calculator (http://pngu.mgh.harvard.edu/~purcell/gpc) (Purcell et al., 2003). To reduce experimental error, the effective sample size was adjusted (calculated sample size×100/95). We calculated sample powers for the SNPs to confirm the effects. To account for multiple testing, the Bonferroni method was used (Bland & Altman, 1995), giving a significance level of α/κ=0.00076 for each test.
Clinical characteristics were compared between control and case subjects, using Student's unpaired t-test for continuous variables with normal distribution including systolic blood pressure (SBP), diastolic blood pressure (DBP), fasting plasma glucose, HbA1c, TG, total cholesterol, HDL-C, and LDL-C. In addition, the statistical significance of association between the genetic variants and clinical characteristics in both the control and case groups was assessed using one-way analysis of variance (ANOVA) with subsequent Tukey's tests. For all of the statistical tests, the level of significance was set at 0.05.
Results
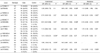
All of the measured clinical characteristics differed significantly between the case and control groups (Table 1). We analyzed the association between each genotype and susceptibility to obesity using logistic regression analysis, after adjusting for age and gender. The genotype distributions of all SNPs selected were in Hardy-Weinberg equilibrium (P>0.05). Of these, seven SNPs (g.+75186C>T, g.+78350C>A, g.+80646C>T, g.+138004C>T. g.+185219G>A, g.+191272A>C, and g.+265317T>A) were significantly associated with the risk of obesity (P<0.05; Table 2). The minor allele of g.+75186C>T, g.+138004C>T, g.+185219G>A, and g.+191272A>C had a protective effect in the dominant (P=0.029, OR=1.68, 95% CI=1.05-2.69), recessive (P=0.05, OR=1.75, 95% CI=1.00-3.05), codominant (P=0.034, OR=1.51, 95% CI=1.03-2.21), codominant (P=0.035, OR=1.68, 95 % CI=1.04-2.72) models, respectively. Conversely, the minor allele of g.+78350C>A and g.+265317T>A showed susceptibility to the risk of obesity when a recessive model was applied (P=0.007, OR=0.46, 95% CI=0.25-0.83, and P=0.02, OR=0.14, 95% CI=0.02-1.12, respectively). In addition, g.+80646C>T was statistically associated with obesity in all models. However, this association disappeared after correcting for multiple testing by the Bonferroni test.
Fifteen LD blocks in PBX1 were constructed using the Gabriel method. (Gabriel et al., 2002) Of these blocks, six LD blocks containing seven significant SNPs were used for further haplotype association analysis. Haplotypes 1 (CAC) and 3 (TAC) of block 3, which consisted of g.+80646C>T, g.+87440A>G, and g.+91850C>T, showed a significant association with obesity in the dominant (P=0.007, OR=0.45, 95% CI=0.26-0.81) and codominant (P=0.027, OR=1.54, 95% CI=1.05-2.25) models, respectively (Table 3). Haplotype 2 (GGAAT) of block 10, which comprised of g.+185286G>A, g.+185602G>A, g.+191125A>G, g.+191272A>C, and g.+194899G>T, was also significantly associated with the risk of obesity in the codominant (P=0.029, OR=1.59, 95% CI=1.05-2.42) and recessive (P=0.034, OR=1.64, 95% CI=1.04-2.59) models. However, when Bonferroni's correction for the multiple comparisons was strictly applied, no haplotype also remained significant in terms of the association with obesity.
For the association analysis of obesity-related phenotypes, we assessed whether the obesity-related phenotypes differed between the two groups (case and control) according to the PBX1 polymorphisms. There were significant differences in SBP, DBP, TG, total cholesterol, HDL-C, and LDL-C, except fasting plasma glucose and HbA1c, between the control and case group for the g.+185219G>A and g.+191272A>C (Table 4). In the control group, subjects that carried the minor allele had higher HDL-cholesterol level compared to the homozygote for the major allele for both g.+185219G>A and g.+191272A>C (59.8 ± 14.9 vs 54.3 ± 10.9 and 61.3 ± 15.3 vs 55.3 ± 11.9, respectively, P<0.001). As shown in Table 1, HDL-cholesterol level was significantly lower in the case group compared to the control group (49.8 ± 11.3 vs 56.9 ± 13.1, P<0.001). Therefore, these results suggest that the association between the homozygote for the major allele for both g.+185219G>A and g.+191272A>C and HDL-C was attributable to an increased risk of obesity.
Discussion
Obesity is a common complex disease that involves multiple genetic variants interacting with environmental and behavioral factors, and is associated with an increased risk of developing insulin resistance and type 2 diabetes. PBX1 gene, comprised of nine exons spanning over 285 kb, maps to a region of chromosome 1 that shows well-replicated linkage to type 2 diabetes in multiple ethnic groups. Several studies support an association between PBX1 polymorphisms and type 2 diabetes mellitus (Elbein et al., 1999; McCarthy, 2003; Ng et al., 2004; Thameem et al., 2001; Xiang et al., 2004). In this study, we evaluated the gene as a possible candidate gene for obesity based on the close relationship between obesity and type 2 diabetes. Our results suggest that some SNPs in the PBX1 gene contribute to obesity and metabolic alterations in a Korean population. In a case-control analysis, of the 66 SNPs examined in PBX1, seven SNPs (g.+75186C>T, g.+78350C>A, g.+80646C>T, g.+138004C>T, g.+185219G>A, g.+191272A>C, and g.+265317T>A) were significantly associated with the risk of obesity. Moreover, haplotypes 1 (CAC) and 3 (TAC) of block 3, consisted of g.+80646C>T, g.+87440A>G, and g.+91850C>T, and haplotype 2 (GGAAT) of block 10, comprised of g.+185286G>A, g.+185602G>A, g.+191125A>G, g.+191272A>C, and g.+194899G>T, of the PBX1 gene had a significant association with the risk of obesity. To our best knowledge, this is the first demonstration that PBX1 polymorphisms are associated with susceptibility to obesity.
Interestingly, a strong association was also found between some SNPs and the HDL-C level in the control group. Control subjects that possessed minor allele g.+185219G>A and g.+191272A>C had higher HDL-C levels. Therefore, the minor allele g.+185219G>A and g.+191272A>C may decrease the risk of obesity. Recently, although there were many reports about individual gene polymorphisms on HDL-C levels (Chien et al., 2008; Kitjaroentham et al., 2007), to our knowledge, this is the first report on the association between PBX1 polymorphisms and HDL-C levels.
We uncovered several intriguing associations between the PBX1 polymorphisms and obesity and related alterations. Nevertheless, our study has several limitations. First, many gene variants contribute to obesity and related alterations and those in PBX1 may have modest effects, requiring large sample sizes to detect associations (Hirschhorn & Daly, 2005). Our sample size was small, and it is possible that the associations that we observed between PBX1 SNPs and obesity could represent false positives. In our study, the power of the sample size was calculated using a genetic power calculator. Our sample provides the power more than 80% to detect more than 1.7-fold increased risk assuming an α-level of 0.05. Thus, our case-control study was sufficiently powerful to determine a positive association. Second, all SNPs selected in PBX1 are located in introns and do not cause an amino acid change. According to the dsSNP database (http://www.ncbi.nlm.nih.gov/SNP/) and the HapMap database (http://www.hapmap.org/), five SNPs in exons of PBX1 gene were reported, but there are unknowns about heterozygosity of them. For this reason, we excluded SNPs present in exons in our study. We suggest that significant polymorphisms in introns may be a marker rather than a direct contributor to the genetic functions. The effects of other genetic variations linked to these polymorphisms may have functional significance. However, we cannot exclude a possibility that these intronic polymorphisms have a role on its genetic function via the change of alternative splicing (Ast, 2004).
In conclusion, our findings suggest that polymorphisms in PBX1 gene might be one of the genetic factors for the risk of obesity, especially in association with alteration of HDL-C level, in a Korean population. Further studies are needed to explore the specific association between g.+185219G>A and g.+191272A> and HDL-C.


 XML Download
XML Download