

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Soy and soy products have been studied in menopausal women for decades. Soy isoflavones are structurally similar to 17 β-estradiol, the primary female sex hormone. It is expected that isoflavones supplement will improve menopause-related health outcomes [1]. However, the question remains whether isoflavones have effects on climacteric symptoms, bone biochemical markers, and menopause-related quality of life.
Previous studies have shown that climacteric symptoms including hot flashes were improved in the isoflavones group compared to the placebo group [234]; in contrast, other studies showed no benefit to isoflavones over placebo [56]. Similarly, their effects on markers of bone turnover have shown contradicting results [7891011]. Although estrogen deficiency negatively impacts women's quality of life by changes in vasomotor, psychosocial, physical, and sexual domains [12], few studies [13141516] have found significant effects of isoflavones on menopausal-related quality of life.
From the previous randomized controlled trials (RCTs) are difficult to generalize to all women because of the diversity in the examined population (racial/ethnic), the variety of isoflavones supplements and dose used (30-120 mg/day isoflavones), duration of exposure (12 weeks-6 months), study design, and responsiveness in postmenopausal women to isoflavones supplementation [16].
Dietary isoflavones intake among Korean adults is 23.1 mg [17], which is 10-20 times higher than that in Caucasian women, or the US or UK adults (0.5-2 mg) [181920]. Until now, there are no study for effect of the isoflavones supplementation on menopausal symptoms in postmenopausal Korean women. Korean women also experience fewer and less severe menopausal symptoms compared to women in Western countries; therefore, the efficacy of soy isoflavones in postmenopausal Korean women must be evaluated.
Therefore, we examined the effects of 70 mg/day isoflavones on climacteric symptoms such as hot flashes, bone metabolism, and quality of life in postmenopausal Korean women with mild climacteric symptoms.
SUBJECTS AND METHODS
Study design
This study was a randomized, double-blind, controlled clinical trial performed over 12 weeks. The study protocol was approved by the Kyung Hee University Hospital Ethnic Committee (Seoul, South Korea) (No: KMC IRB 1002-02). The trial was performed according to the Declaration of Helsinki and was in accordance with the principles of Good Clinical Practice. This trial was registered with Clinical Research Information Service (Number KCT0001737). The Clinical Research Information Service is a non-profit online registration system for clinical trials to be conducted in Republic of Korea by established at the Korea Centers for Disease Control and Prevention [21].
Subjects
Eligible subjects were postmenopausal women with mild menopausal symptoms aged 45-60 years, with BMI ranging from 19.0 to 30.0 kg/m2. Postmenopause was defined as a last menstrual period > 12 months ago prior and serum follicle-stimulating hormone (FSH) level > 40 IU/mL. Mild menopausal symptoms were defined by a Kupperman index ranging from 20 to 40 and hot flashes for at least three months. Women were excluded if they received hormone replacement therapy or selective estrogen receptor modulators within three months of enrollment or had a history of breast or genital tract malignancies or vascular disease. Women with abnormal findings such as endometrial proliferation, endometrial cancer, uterine cervical cancer, and breast cancer-related conditions on clinical examination, ultrasound of the pelvis and abdomen, or breast X-ray were excluded. Patients with cardiovascular disease, kidney disease, thyroid disease uncontrolled hypertension (≥ 170/100 mmHg), or diabetes (≥ 180 mg/dL) were excluded. Women with depression, schizophrenia, alcohol abuse, or other drug abuse were also excluded.
Subject sample planning and study power
To sample size estimation, we used similar study [22], hot flashes as a primary outcome were significantly reduced in the isoflavones group (score from 7.0 ± 1.8 to 3.4 ± 3.2) compared with in the placebo group (score from 6.4 ± 2.4 to 5.2 ± 2.7). We estimated that a sample of 43 postmenopausal women for each group would be required to detect a difference with a power 80% and a two-sided α level of 5%.
Isoflavones and placebo tablets
The isoflavones tablets were provided by Dr. CHUNG's Food Co. (CHUNG's Food Co., LTD., Cheongju, South Korea). Each tablet (400 mg) contained 336.0 mg of soy extract (isoflavones 10.5%) and various bulking agents, including lactose powder mixture (15.6%), silica dioxide (0.5%), and magnesium stearate (0.5%). The placebo tablets contained dextrin instead of isoflavones. All subjects were instructed to take two tablets daily (corresponding to isoflavones 70 mg/day). The total dose of isoflavones was thus about 70 mg/day in glycoside, which corresponded to 38.0 mg glycitin, 20 mg daidzein, and 12.4 mg genistin. The components of the isoflavones were analyzed and labeled using high-performance liquid chromatographic (HPLC) methods [23]. In Korea, there is no defined isoflavones dosage for improving menopausal symptoms and health outcomes. According to the Japanese Food Safety Commission in 2006, the safe upper limit of isoflavones should be restricted to 70-75 mg/day [24]. Considering that most of the aforementioned studies that showed the effectiveness of isoflavones on menopausal symptoms were conducted using 70 mg/day, we restricted dietary isoflavones intake in our study. During the supplemental period, isoflavone intake from foods was restricted to less than 10 mg/day. All women received education on dietary isoflavones sources (such as soybean, soy milk, peanut, bean sprout, miso, soybean curd, uncurdled bean curd, soybean curd residue, and fried soybean curd) and replacement methods (for example, soy milk or bean sprout can be replaced by milk or other vegetables) [252627] by a dietician using education materials and a one-on-one. The daily consumption of isoflavones from foods did not differ between groups at baseline and after 12 weeks; however, there were significant differences within groups (isoflavones group: from baseline 18.8 ± 14.2 mg to 3.4 ± 3.7 mg, P < 0.0001 and placebo: from baseline 16.8 ± 17.0 mg to 4.0 ± 5.1 mg, P < 0.0001, respectively).
Trial protocol
Participants were recruited through a variety of outreach methods such as posters, word of mouth, presentation at community center, and website advertisements. At the screening visit (-1 week), postmenopausal women provided written informed consent and were assessed for eligibility through a screening mammogram and clinical blood chemistry measures. Individual information was collected by trained interviewers via face-to-face interview based on structured questionnaires on sociodemographic data, medical history, medications, dietary habits, and physical activity. At the baseline visit (0 week), postmenopausal women who met the study criteria were randomly assigned to either the isoflavones or placebo group. Randomization was performed according to a computer-generated random list. All investigators, research staff, and subjects were blinded to the treatment codes. After the baseline visit, women returned at the inter-visit (6 weeks) and final visit (12 weeks) to complete surveys on Kupperman index and menopause-specific quality of life (MENQOL) and for monitoring of adverse effects. Subjects were required to discontinue the use of other dietary and herbal supplements and minimized the intake of food sources of isoflavones < 10 mg/day, which were monitored by 3-day food diaries. Compliance with the isoflavones and placebo was assessed by pill counts of empty pill blister packs and the remaining pills at the 6- and 12-week visits and was calculated using the following formula: (number of tablets dispensed - number of tablets returned/number of tablets subject was expected to take) × 100.
Analysis of blood parameters
Blood samples were drawn from a mid-arm vein following an overnight fast at the baseline and final visits of the study. Obtained samples were separated into ethylenediamine tetra-acetic acid-potassium anticoagulant tubes and serum-separate tubes (SSTs). SSTs were immediately centrifuged (3,000 × g, 4℃, for 10 min), and the supernatant was used for analysis. For bone formation markers, the serum levels of osteocalcin (OC) and bone-specific alkaline phosphatase (BALP) were analyzed using Clinical Laboratory Improvement Amendments or radioimmunoassay using a commercial kit. For bone resorption markers, N-terminal telopeptide of type I collagen (NTx) was measured using an enzyme linked immunoassay kit (Osteomark, Wampole Laboratories, Princeton, NJ, USA), and urinary-deoxypyridinoline (u-DPD) was measured with a commercial enzyme immunoassay kit (Metra DPD ElA Kit, Quidel Corporation, USA) with in-run CVs of 4.3-8.4% and between-run CVs of 3.1-4.8%. Values were corrected based on urinary creatinine (Cr) level for standardization (Dpd / Cr). The concentration of urinary Cr was measured using an Auto Analyzer ADVIA 1650 (Bayer, Tokyo, Japan).
Climacteric symptoms and hot flash measurements
Scores of climacteric symptoms and hot flashes were measured by Kupperman index [28]. The Kupperman index included sweating/hot flashes, palpitations, vertigo, headaches, paresthesia, formication, arthralgia, myalgia, fatigue, nervousness, melancholia, urinary infection, and sexual complaints. A scale ranging from 0 to 3 points was used to describe the severity of the complaints. The weighting factors were the same as those used in the original Kupperman index and assign two points for the urogenital symptoms. Scores ranging from 0-20, 20-40, 40-60, and 60 were used to rate the degree of severity as none, mild, moderate, and severe, respectively. Hot flash scores were subjectively graded on a scale (0 = not at all, 1 = weak, 2 = moderate, 3 = severe symptoms), and weighting was achieved by multiplying the score of hot flashes by 4, with a maximal score of 12.
Menopausal-specific quality of life measurements
Quality of life was measured by the MENQOL questionnaire [29], developed as a condition-specific, self-completed outcome tool to assess the impact of menopause and to evaluate interventions. The MENQOL includes 29 items divided into four domains of vasomotor (3 items), psychosocial (7 items), physical (16 items), and sexual (3 items). A seven-point Likert scale ranging from 0 (not at all bothered) to 6 (extremely bothered) was used. Once each item was reported as a 0-6 score, each domain was scored by averaging the reported values. Hence, the average for each domain was between 0 (not at all a problem; respondent selected “no” for each item in the domain) and 6 (respondent reported experiencing each symptom in the domain at the highest degree of bother).
Statistical analysis
Statistical analysis was performed using Statistical Package of Social Sciences (SPSS, IBM Cooperation, Chicago, IL, USA) version 21.0. The categorical variables of the two groups were compared with the Chi-square test, and the data are presented as percentage (%) or number (n). For non-parametric data, the distribution of variables was assessed using the Kolmogorov-Smirnov or Shapiro-Wilk tests for normality and the F-test for homogeneity of variances. When allowed by data distribution and homogeneity of variances, the independent or paired t-test was performed to evaluate the significance between groups or within a group. In addition, repeated-measures ANOVA was performed to test the significant group × time effects of isoflavones on menopausal symptoms and MENQOL scores during the treatment period. The Bonferroni test was used for post hoc multiple comparisons. A two-tailed P-value less than 0.05 was considered statistically significant for all analyses.
RESULTS
Subjects
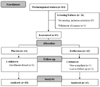
Of the 113 women considered for the study, 25 were excluded due to a serum level of FSH less than 40 IU/mL and 1 for withdrawal of consent. Of the 87 postmenopausal women randomized into the trial, 1 in the placebo group and 2 in the isoflavones group did not reach the end of the trial; hence, there were 43 in the placebo group and 41 in the isoflavones group with at least baseline data available for analysis. The flow of subjects through each stage of the trial is detailed in Fig, 1, as based on recommendations made in the Consolidated Standards of Reporting Trials statement [30].
Sociodemographic & health-related behaviors
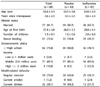
There were no significance differences in sociodemographic or health-related behaviors between groups (Table 1). Age and years since menopause of the placebo and isoflavones groups were similar (P = 0.6776, P = 0.8928). Most women had a high school education (73.8%) and were married (91.7%). The number of subjects who exercised regularly was 69.8% in the placebo and 70.7% in the isoflavones group. The number of subjects who smoked or drank alcohol was not significantly different between the groups.
Kupperman index including hot flashes
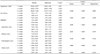
There was no significant difference in Kupperman index including hot flashes at baseline. At 12 weeks, the Kupperman index was reduced in both groups, −7.0 ± 15.8 (P = 0.0074) in the isoflavones group and −6.3 ± 14.4 (P = 0.0064) in the placebo from baseline. The score for hot flashes was also significantly reduced in both groups, −2.0 ± 2.4 in the isoflavones group and −2.7 ± 3.0 in the placebo group from baseline (P < 0.05). No interaction of dose × time effects was shown (Table 3).
Markers of bone formation and resorption concentrations
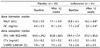
At baseline, OC was significantly lower in the isoflavones group, while the other bone parameters were similar between two groups (Table 2). After 12 weeks, the bone formation markers BALP and OC significantly increased by 6.3 ± 4.1% (P = 0.004) and 9.3 ± 6.2%, respectively. Serum BALP level increased in the isoflavones group (form 14.8 ± 4.5 U/L to 16.2 ± 4.8 U/L) compared to the placebo group (from 16.0 ± 5.9 U/L to 16.0 ± 5.9 U/L). Serum OC level increased in the isoflavones group (from: 7.7 ± 2.8 pg/mL to 9.1 ± 2.4 pg/mL) compared to the placebo group (placebo: 9.2 ± 3.3 pg/mL; isoflavones: 9.1 ± 2.6 pg/mL). Bone resorption markers, urinary DPD and serum CTX concentration, did not changed regardless of group during the treatment period.
Menopausal-specific quality of life
No significant difference was noted in overall average MENQOL score between groups at baseline (isoflavones group: 1.0 ± 0.6 and placebo: 1.3 ± 0.8). After 12 weeks, the data showed significant changes both between the two groups (P = 0.0228) and within the groups. The final scores were placebo group: 0.6 ± 0.4, P < 0.0001 and isoflavones group: 0.6 ± 0.5, P < 0.0001. There was an effect of the interaction of dose ×time (P = 0.048) (Table 3).
The subscale score for MENQOL was 1.51 ± 1.42 for vasomotor, 0.80 ± 0.62 for psychosocial, 0.89 ± 0.59 for physical, and 1.56 ± 1.64 for sexual in the isoflavones group. After 12 weeks, the scores decreased to 0.75 ± 1.02 (−0.76 ± 1.13 change) for vasomotor, 0.48 ± 0.50 (−0.32 ± 0.52 change) for psychosocial, 0.51 ± 0.49 (−0.38 ± 0.5 change) for physical, and 0.91 ± 1.40 (−0.65 ± 1.21 change) for sexual in the isoflavones group.
The subscale score for MENQOL was 1.65 ± 1.06 for vasomotor, 1.22 ± 1.02 for psychosocial, 1.18 ± 0.79 for physical, and 2.08 ± 1.73 for sexual in the placebo group. After 12 weeks, the scores decreased to 0.42 ± 0.59 (−1.23 ± 1.03 change) for vasomotor, 0.58 ± 0.59 (−0.63 ± 0.98 change) for psychosocial, 0.54 ± 0.48 (−0.64 ± 0.73 change) for physical, and 0.95 ± 1.04 (−1.12 ± 1.68 change) for sexual in the placebo group.
DISCUSSION
Our study is the first report that isoflavones supplementation have benefit on bone biomarkers, although the results are ambiguous for menopausal symptoms and MENQOL among Korean postmenopausal women. Daily dietary supplementation with 70 mg isoflavones was effective for alleviating hot flashes and Kupperman index at 6 and 12 weeks compared to baseline, although no significant difference was noted between groups. Interestingly, the Kupperman index score at 6 weeks in the isoflavones group was significantly decreased, while that in the placebo group did not change. After 12 weeks, both the isoflavones and placebo groups showed a significant decrease in Kupperman index. Also, isoflavones increased the levels of the serum bone formation markers, BALP and OC, in line with previous results. MENQOL decreased at 6 and 12 weeks in both groups, and there was a significant different between groups, with changes in the placebo group being greater than those in the isoflavones group.
Various assessment tools for hot flashes and menopausal symptoms exist, and we used the Kupperman index, a tool that provides severity score via a composite score that multiplies the number of hot flashes by their severity, graded from 1 to 3. In early postmenopausal Chinese women (n = 90, aged 45-60 years), the frequency of hot flashes and the Kupperman index score were previously shown to decrease for different dose interventions (44.3 ± 19.1 and 57.8 ± 37.4 [84 mg isoflavones]; 48.5 ± 27.2 and 56.7 ± 26.7 [126 mg isoflavones]) compared to the placebo group (27.8 ± 15.5 and 34.6 ± 46.2; P < 0.01) [31]. Compared with our study, the previous study used a single-blinded design, which may have introduced observational biases, particularly in subjective outcomes [31]. The effects of isoflavones may be influenced by the baseline frequency of hot flashes, with a higher frequency leading to greater efficacy [32]. For example, Nahas et al. [2] studied a total of 80 Brazilian women (mean age: 55.1 years), who reported 5 or more hot flash episodes per day, and found that, after 10 months, isoflavones (100 mg/day) were significantly superior to placebo in reducing hot flash severity (69.9% and 33.7%, respectively). Ferrari et al. [3] evaluated 180 women (aged 40-65 years) with a minimum of 5 moderate-to-severe hot flashes in the 7 days and who had experienced no menstruation for at least 6 months, treated them for 12 weeks with 80 mg of isoflavones daily, and showed that the reduction was greater in the isoflavones group at 6 (36.2%) and 12 weeks (41.2%) than in the placebo group (24.0% at 6 weeks, 29.3% at 12 weeks).
The significant increases in the bone formation markers BALP and OC after 12 weeks are in line with a meta-analysis of RCTs that showed that isoflavones significantly increased serum BALP by 20.3% when used at a 75 mg/day dose [33]. Although we cannot provide an exact mechanism for how soy isoflavones lead to favorable effects on bone metabolism, there is some evidence. First, Morabito et al. [34] suggested that genistein, in contrast with estradiol, increases as a bone formation marker in postmenopausal women. Second, Choi et al. [35] and Kannoa et al. [36] showed in vitro study effects of isoflavones that likely involve recruitment and differentiation of osteoblastic precursors that result in increased osteoblast-mediated bone formation and increased bone mass in a dose-dependent manner. Third, soy isoflavones stimulate osteoblastic activity through activation of estrogen receptors and promotion of insulin-like growth factor (IGF-1) production; in turn, IGF-1 enhances osteoblastic activity in humans [37].
However, our results did not changes in bone resorption markers in contrast with a previous study that soy or isoflavones intake decreased DPD [121314151617]. In accordance with our results, soy protein 40 g (approximately 118 mg/day of isoflavones) for 12 weeks resulted no significant differences with a placebo group in u-DPD concentration (Isoflavones:−0.8 ± 0.9 vs. Placebo:−0.3 ± 0.7 nmol/mmol Cr, P = 0.40) [38]. Isoflavones dosage, duration, and various other factors such as the medium of administration, chemical form, metabolism, bioavailability, level of exposure, and the hormonal and dietary states of the individual may affect bone metabolism. For example, isoflavones have different effects on women who are equol or non-equol producers [39]. Non-equol-producing women may not benefit from isoflavones because they may lack the enzyme or bacterium in their intestine that converts daidzein into equol, which resembles 17β-estradiol, and has a higher affinity for both estrogen-binding sites in blood vessels [40]; notably, Asian populations have higher rates of equol producers than white populations. The percentage of equol producers was 56% in postmenopausal Japanese women [31] compared with only 28% in the United Kingdom [32]. In postmenopausal Japanese women (n = 93, mean age: 55 years), u-DPD was significantly decreased, with a 23.9% change in the group that received 10 mg/day of equol supplement compared with a 2.9% change in the placebo group (P = 0.020) [43]. In our study, we did not evaluate equal status, a possible limitation of our study.
In our study, the average years since menopause was within 5 years, which may be related to the low MENQOL scores at baseline (28.7 ± 18.4 isoflavones vs. 38.4 ± 24.2 placebo). It is possible that participants with higher MENQOL score would have derived some benefit. It is also possible that women in early menopause, when vasomotor menopausal symptoms tend to be most frequent, would have derived some benefit. Factors such as the number of years since menopause and body weight affect hot flash frequency, menopausal symptoms, bone remodeling, and menopausal-related quality of life. In our sub-analysis, stratified for years since menopause (early ≤ 3.5 y, late > 3.5 y) and BMI (normal as BMI < 23 kg/m2, overweight as BMI ≥ 23 kg/m2), there were no significant differences between groups (Tables 4, 5).
Our study has several limitations. A primary limitation was the high placebo response rate (maximum 50.0%). In a pooled analysis of 10 RCTs of hot flash treatment, the placebo response rate ranged from 27 to 52% [44]. Our study suggest considered to the more specific inclusion criteria; the US Food and Drug Administration recommends inclusion of subjects that have hot flashes with a frequency of at least 7 per day and a treatment period of 12 weeks [45]. Also, to assess the placebo response, we considered study designs such as “balanced placebo design” and the “balanced cross-over design” [46]. Another limitation is that the Kupperman index and MENQOL questionnaire are self-reporting questionnaires; women were asked to provide some retrospective information such as climacteric symptoms experienced in the preceding weeks; thus recall bias was unavoidable. Finally, we did not measure serum isoflavones changes, which should be analyzed in a further study as a compliance indicator.
Despite these limitations, our study showed excellent compliance among the 84 women (96.8% achieved 80% compliance) with strictly limited soy-containing food supplementation over the study period.
Our findings suggest that isoflavones supplements have a beneficial effect on the bone formation markers BALP and OC in Korean postmenopausal women. Evaluation of the effects of isoflavones on improvement in hot flashes, climacteric symptoms, and quality of life need to be further studied with strict subject inclusion criteria.


 XML Download
XML Download