

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Lung cancer is one of the leading cancer deaths throughout the world. Despite major advances in cancer treatment, during the past two decades, lung cancer carries a very poor prognosis, and the overall 5-year survival rate has remained less than 15% (1).
Although tumor, node and metastasis stage is the most significant prognostic parameter to be considered, the variability of survival within the staging groups requires additional parameters, which influences the outcome, independent of stage factors.
The molecular alterations in lung cancer have been extensively studied (2). They consist mainly of inactivating the mutations of tumor suppressor genes, activating mutations of oncogenes, loss of heterozygosity, and amplification of chromosomal regions. Recent progress in the study of the molecular biology of cancer has contributed to a better understanding of its molecular pathogenesis, including that of lung cancer. Cell proliferation is regulated by many factors. Recent studies have shown that cyclins and cyclin-dependent protein kinase (cdk) complexes have important roles, during the cell cycle progression (3,4). Regulatory mechanisms include variations in cyclin abundance, phosphorylation of the kinase sub-unit that may yield either positive or negative effects, or the actions of cyclin-kinase inhibitory proteins. The complex formed by cyclin D1 and cdk4 governs the G1 progression, while cyclin E and cyclin A in connection with cdk2, regulates the entry to and progression through the S phase (5). In this investigation, they analyzed the prognostic value of cyclin A, cyclin D1, cdk2, and cdk4 in patients with squamous cell carcinoma of the lung. Cyclins D and E are relatively recently described proteins that are implicated in the pathogenesis of non-small cell lung carcinomas (NSCLCs). Cyclins and their associated cyclin-dependent kinases regulate progression of the cell cycle, through the G1 phase and into the S-phase of the DNA replication process (4). Overexpression of cyclin D1 and cyclin E has been demonstrated to shorten the G1 phase of the cell cycle (6).
Studies examining the use of immunohistochemical staining for cyclins, as a potential prognostic marker, are rare. Overexpression of cyclin D1 and cyclin E has been reported in several tumors, such as colorectal, head and neck, esophageal, breast, uterus, hepatocellular, in addition to lung carcinoma, melanomas, and sarcoma (7).
In the present study, we have used immunohistochemical techniques to analyze the overexpression of cyclins in human NSCLCs to elucidate the potential role in tumor development. The relationship to various clinicopathological factors was then determined.
MATERIALS AND METHODS
1) Patients and tissue samples
A total of 103 formalin-fixed, paraffin-embedded lung cancer specimens were obtained from patients who underwent a surgical resection (lobectomy or pneumonectomy) in Gachon University Gil Hospital and Korea University Hospital, between 1997 and 2001. The patients with NSCLCs consisted of 84 men and 19 women, with mean age of 63 years (range, 41~85 years). The histologic classification of the tumor specimens was based on World Health Organization (WHO) criteria and the specimens included 68 squamous cell carcinomas, 25 adenocarcinomas, 8 large cell carcinomas, and 2 adenosquamous cell carcinomas. They represent 1 for stage 0, 14 for stage IA, 28 for stage IB, 9 for stage IIA, 27 for stage IIB, 23 for stage IIIA, and 1 for stage IIIB.
2) Immunohistochemistry
A total of 103 lung cancers were fixed in 10% buffered formalin and embedded in paraffin, and cut to approximately 4µm thick sections. These sections were deparaffinized in zylene, dehydrated, placed in methanol containing 5% hydrogen peroxide for 5 minutes at room temperature, autoclaved in citrate buffer (pH 6.0) at 132℃ for 12 minutes. Subsequently, incubation with monoclonal antibody to cyclin A, B1, D1, D3, or cyclin E antigen was carried out or 24 hours at 4℃. Monoclonal antibodies against human cyclin E protein (NCI-cyclin E, clone 13Ae) and human cyclin D1 protein (NCL-cyclin D1-GM, clone P2D11F11) were purchased from Novocastra (Newcastle, UK). Anti-cyclin E antibody was diluted at 1:50, and anti-cyclin D1 antibody was diluted at 1:20. The slides were washed, incubated with biotinylated goat anti-mouse immunoglobulin G antibody, and incubated with avidin-biotin-peroxidase complex for 10 minutes, using a streptavidin-biotin complex peroxidase kit (Large Volume DAKO LSAB kit; Dako, Glostrup, Denmark). Afterwards, the chromogen 3, 3'-diaminobenzidine tetrahydrochloride was applied for 10 minutes and weak counterstaining was carried out with Mayer's hematoxylin.
The number of tumor cells with nuclear immunopositivity was graded on a scale of: 0, less than 1%; 1, 1 to 30%; 2, 30 to 60%; and 3, more than 60%. Histologic subtype, stage, and age, gender were correlated with grade of immunohistochemical staining.
RESULTS
The patients ranged in age from 41 to 85 years, at the time of diagnosis, with a mean age of 63.1 years. The male and female patients were 84 and 19, respectively. Tumor size was 1 cm to 12 cm. The average was 2.1 cm. Tumor was located on the right for 64 cases (62.1%) and on the left for 39 cases (37.9%). The number of lymph node metastasis was 69. The visceral pleural invasion was seen in 19 cases. Thirteen cases showed both pleural invasion and lymph node metastasis (Table 1).
Histological subtypes included 68 squamous cell carcinomas, 25 adenocarcinomas, 8 large cell carcinomas, and 2 adenosquamous cell carcinomas.
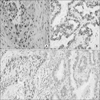
Positive immunostainings of cyclin A, B1, D1, D3, and E were confined to nuclei of cancer cells in every case. Most tumor stroma and accompanying inflammatory cell were negative. The overexpression of staining was estimated over score 2. The positive immunoreactivity was observed in 51 cases (50%) for cyclin A, 33 cases (32%) for cyclin B1, 83 cases (81%) for cyclin D1, 19 cases (18%) for cyclin D3, and 11 cases (11%) for cyclin E (Fig. 1). The expression of cyclin A and D1 represented more than 50% all of NSCLCs. However, that of cyclin B1 was frequently observed in squamous cell carcinoma (30/68, 44%), compared to that of adenocarcinoma (2/25, 8%), which was not significant for statistical analysis. Cyclin E positivity was frequently found in large cell carcinoma (2/8, 25%), compared to that of squamous cell carcinoma (8/68, 11%) and adenocarcinoma (1/25, 4%). There were no significant differences of the expression of cyclin A, B1, D1, and D3, according to the following parameters: sex, tumor size, histological types and tumor different ion. Only cyclin E expression was correlated with lymph node metastasis (p<0.004). It was the immunohistochemical data subdivided by histologic subtype, stage, and percent of tumor cells, as seen in Table 2.
DISCUSSION AND CONCLUSION
Lung cancer is a major cause of mortality, worldwide. To further improve the survival rate in this group of patients, their prognostic classification, which is based on tumor biology, will be crucial. Such classification might help clinicians to make the right management decisions for each subset of patients.
Altered regulation of the cell cycle is a hallmark of human cancers (8). Cell cycle progression is governed by a series of cyclins and cdks. Individual cyclins act at different phases of the cell cycle by binding and activating the corresponding cdks. Of the various cyclin/cdk complexes that are involved in the cell cycle regulation process, cyclin D1/cdk4/6 and cyclin B1/cdc2 are of particular interest, since the former directs the G1-S-phase transition and the latter controls the G2-M-phase checkpoint surveillance, which are in turn essential for DNA synthesis and cell proliferation. Dysregulated expression of these cyclins, cdks, or both, may lead to uncontrolled cell growth and malignant transformation. Cyclin B1 is a key molecule for G2-M-phase transition, during the cell cycle, and is overexpressed in various tumor types. Overexpression of cyclin B1 has been reported more recently in breast, colon, prostate, oral, and esophageal carcinomas (9-13). Soria et al. (14) has shown, using a homogeneous population of 77 patients with stage 1 NSCLC, that there is an overexpression of cyclin B1 in lung tumors, particularly in squamous cell carcinoma, and that such overexpression was associated with patients' prognosis. However, the expression status of cyclin B1 in lung cancer and its clinical significance remains unknown. We couldn't demonstrate the correlation with cyclin B1 and clinical-histologic factors.
There were some studies that have evaluated the clinical significance of cyclin D1 and E expression in NSCLCs. Overexpression and/or amplification of cyclin D1 has been reported in a large variety of human cancers, including those of the esophagus, head and neck, lung, liver, and breast (4) and is reported to be of prognostic importance in patients with most of these tumor types (15,16). These studies have suggested that overexpression of cyclin D1 shortens the G1 phase and accelerates cell growth, thus, positively contributing to oncogenesis. Cyclin E overexpression has also been observed invarious human carcinoma cell lines and tumor tissues, such as breast cancer, gastric carcinoma, colorectal adenoma and colorectal adenocarcinoma (17). The rates of cyclin D1 expression in NSCLCs were between 18% and 55.5%, in previous studies. Our present study was 81%, which was slightly higher in comparison with other studies. However, there was a conflict regarding the role of overexpression of cyclin D1 in relation to pathological findings and prognosis (18). Overexpression of cyclin E becomes more severe with tumor stage and grade, and is consistent with proliferative activity (17) in this study, high cyclin E expression was significantly associated with lymph node metastasis. It might result in unfavorable prognosis. Several reports represent that cyclin E expression has been demonstrated in association with advanced tumor stage, increasing grade, and unfavorable prognosis in breast cancer (19).
In summary, we have demonstrated the high cyclin E expression represented correlation with lymph node metastasis and was an unfavorable prognostic factor. Cyclin E might be a potential neo prognostic factor of NSCLCs.


 XML Download
XML Download