

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Lung cancer is the most common cause of cancer-related mortality in the world today. Primary lung cancer has been classified into 2 clinically relevant groups: small cell lung carcinoma (SCLC) and non-small cell lung carcinoma (NSCLC). This distinction was clinically useful as available treatment strategies differed significantly between these 2 groups. More recently, the identification of molecular differences between specific subtypes of NSCLC and the emerging evidence for differential responses to new targeted therapies has necessitated greater accuracy in the subtyping of NSCLC. Adenocarcinoma (ADC) and squamous cell carcinoma (SCC) are the 2 major subtypes of NSCLC. Recent clinical trials for NSCLC revealed that some chemotherapeutic regimens (e.g., pemetrexed) were apparently more effective for non-SCC than for SCC (1), while other agents (e.g., bevacizumab) were of limited use for SCC because of fatal pulmonary hemorrhage risks (2). Moreover, the ADC subtype is more predictive of a better response to epidermal growth factor receptor inhibitors, especially in Asian women who have never smoked (2). Consequently, accurate histologic typing of NSCLC is essential when formulating treatment therapies (3).
Many NSCLC are heterogeneous and show areas of undifferentiated tumor that lack the light-microscopic features of differentiation visible in other parts of the lesion. The combination of a small diagnostic sample size and tumor heterogeneity results in a lack of consistency and accuracy in subtyping NSCLCs (4,5). Morphologic separation of poorly differentiated (PD) ADC from PD SCC can be difficult, with low interobserver agreement even among experienced pulmonary pathologists (6). Some studies have found that this diagnosis accounts for up to 25% of NSCLC diagnoses in small biopsy and 45% of cytology samples (7). When PD NSCLC is present in small biopsy sample, a diagnosis of non-small cell lung carcinoma-not otherwise specified (NSCLC-NOS) is recommended (8-10). However, this has led to the used of the NSCLC-NOS diagnosis in more than 30% of histologic and close to 40% of cytologic samples (11). Immunohistochemistry (IHC) can allow tumor subtypes to be inferred when histologic morphology is nonspecific. While none of the markers to date have 100% sensitivity or specificity, most studies have agreed on the inclusion of thyroid transcription factor-1 (TTF-1) as an ADC marker and p63 as an SCC marker. Other markers, such as cytokeratin 5/6 (CK5/6), cytokeratin 7 (CK7), desmocollin-3, high molecular weight cytokeratin (HMWCK), and napsin A, may also contribute to tumor subtyping (12-19).
In this study, we investigated 4 SCC markers (CK5/6, desmocollin-3, HMWCK, and p63) and 3 ADC markers (CK7, napsin A, and TTF-1) using a tissue microarray (TMA) format sampled from resection specimens diagnosed as SCC and ADC to simulate small biopsy conditions. We evaluated the ability of these IHC markers and mucin staining to predict the most likely NSCLC subtype.
MATERIALS AND METHODS
1) Patients and specimens
Between 1985 and 2005, a total of 281 patients (with primary pulmonary ADCs and SCCs) was diagnosed and operated on at Kyung Hee Medical Center (Seoul, Republic of Korea), College of Medicine, Kyung Hee University; all patients were included in this study. Within the sample population, there were 110 patients diagnosed with ADCs and 171 patients diagnosed with SCCs. Patients underwent surgical resection by hilar and mediastinal lymph node sampling. On a retrospective basis, certain clinical and pathologic parameters were summarized from the patient's file, including age, gender, histopathologic type, and tumor differentiation (Table 1). The mean patient age at surgery was 62 years (range, 35~81 years). Standard hematoxylin and eosin (H&E)-stained sections of the formalin-fixed, paraffin-embedded tumor tissues were reviewed by 2 pathologists (G.Y.Kim and S.J.Lim) to confirm the histologic diagnosis according to the current World Heralth Organization (WHO) classification (20). Well to moderately-differentiated ADC (71%) or SCC (83%) was easily recognized as glandular or squamous differentiation. Thirty-two of the 110 (29%) patients diagnosed with ADC and 29 (17%) of 171 patients diagnosed with SCC were PD.
2) Tumor tissue and TMAs
The paraffin embedded tissues were sampled from archived conventional tissue blocks. Three areas of tumor were chosen by 2 surgical pathologists (G.Y.Kim and S.J.Lim). The TMAs were constructed with an AccuMaxTM Array (ISU ABXIS/PeTagen, Seoul, Korea) by sampling 3 representative areas (2.0 mm in diameter) of the original tumor and transferring them into a new array block.
3) IHC and histochemistry
Primary antibodies, sources, and dilutions are listed in Table 2. Antibodies were applied to 4-µm-thick TMA sections using a Bond Polymer Intense Detection System (VisionBioSystems, Mount Wacerley, VIC, Australia) according to the manufacturer's instructions with minor modifications. In brief, each formalin-fixed and paraffin-embedded section had its paraffin removed with Bond Dewax Solution (VisionBioSystems), and was subjected to antigen retrieval using Bond ER Solution (VisionBioSystems) at 100℃ for 30 minutes. The endogenous peroxidase was subsequently quenched by incubation with hydrogen peroxide for 5 minutes. The sections were then incubated for 15 minutes at room temperature with antibodies using a biotin-free polymeric horseradish peroxidase-linker antibody conjugate system in a Bond-maX™ automatic slide stainer (VisionBioSystems), and visualized using a 3.3-diaminobenzidine (DAB) solution (1 mM DAB, 50 mM Tris-HCL buffer [pH 7.6], and 0.006 % H2O2). The slides were counter-stained with hematoxylin. Appropriate positive tissue controls were performed for each immunostain and for mucicarmine histochemical stain, all of which demonstrated appropriate staining patterns, as defined in Table 2. In addition, internal positive controls showed appropriate staining. Parallel negative controls, without a primary antibody, were included for each TMA section and all displayed negligible staining. Mucicarmine staining was performed using standard methods. Sections of each TMA were also stained with H&E using standard methods as an additional histologic reference.
4) Interpretation of histochemical and immunohistochemical staining
Histochemical and immunohistochemical staining were assessed in 5 high powered fields at 400× magnification. CK5/6, CK7, desmocollin-3, HMWCK, napsin A, p63, and TTF-1 immunoreactivity were evaluated semiquantitatively based on staining intensity and proportion (Fig. 1). The stained tumor tissues were scored blindly with respect to clinical patients by 2 investigators (G.Y.Kim and S.J.Lim). Immunoreactivity was scored semiquantitatively by recording the proportion and intensity of immunoreactive tumor cells (16,21). Proportion of immunoreactivity was defined based on 4 categories: score 0, 0%; score 1, 1~9%; score 2, 10~49%; score 3, ≥50% tumor cells. In addition, intensity of immunoreactivity was recorded as follows: score 0, none (absent); score 1, weak (less than normal cells); score 2, moderate (same as normal cells); and score 3, strong (stronger than normal cells). When immunohistochemical scores of duplicate cores are discrepant, the higher score was used. Pneumocytes served as internal controls for TTF-1, napsin A, and CK7 reactivity, and bronchial basal cells for p63, CK5/6, HMWCK (34βE12), and desmocollin-3 reactivity. Histologic (H) scores were derived by multiplying proportion scores (0, 1, 2, and 3) by intensity scores (0, 1, 2, and 3), yielding a number between 0 and 9. We used a dichotomous scoring cut-off value based on receiver operating characteristic (ROC) curve analysis. The diagnosis of ADC required detecting any intracytoplasmic mucin droplets in tumor cells with mucicarmine staining (20).
5) Data analysis
The significance of relationships between tumor differentiation and the H score of immunohistochemical markers were investigated using a Pearson Chi-square test. Sensitivity, specificity, positive predictive values (PPV), and negative predictive values (NPV) were estimated for each marker. The area under the curve (AUC) on ROC curve analysis was used to compare the ability of an antibody to discriminate between SCC and ADC. The AUC ranged between 0.5 (indicating no predictive value) and 1 (indicating perfect predictive accuracy). To estimate the amount of variation to be expected for these values and enhance comparisons to each other and published values, a 95% confidence interval (CI) was estimated. For analyzing the immunohistochemical panels to differentiate between ADC and SCC, we performed multivariate analysis using logistic regression analysis. All tests of significance were 2-sided, and differences were considered statistically significant at a p-value of <0.05. Data analyses were performed using MedCalc for Windows version 12.2.1 (MedCalc Software, Mariakerke, Belgium).
RESULTS
1) Immunohistochemical findings by tumor differentiation
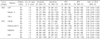
Immunohistochemical findings according to tumor differentiation are present in Table 3. TTF-1 was positive in 75 of 110 (68%) ADCs sampled and in none of the SCCs. Desmocollin-3 was positive in 156 of 171 (91%) SCCs and in none of the ADCs. Desmocollin-3 and p63 had significantly decreased immunoreactivity in PD SCC (59% and 86%). However, p63 immunoreactivity was the highest (86%) among the SCC markers in PD SCC. CK7 immunoreactivity expression was significantly increased in PD SCC (28%).
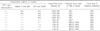
2) Sensitivity, specificity, PPV, NPV, and AUC on ROC of one marker
The sensitivities, specificities, PPV, NPV, and AUC on ROC of the markers for ADC and SCC are presented in Table 4. For ADC, the single most sensitive marker and best negative predictor was CK7 (sensitivity, 95%; NPV, 96%), and the most specific and best positive predictor was TTF-1 (specificity, 100%; PPV, 100%). Napsin A was specific (98%) for ADC and the 95% CI for specificity and PPV overlapped with those of TTF-1. For SCC, p63 is the most sensitive marker and best negative predictor (sensitivity, 96%; NPV, 93%). Desmocollin- 3 was the most specific and best positive predictor (specificity, 100%, PPV, 100%). Among the PD, the same results were found. TTF-1 and desmocollin-3 were mutually expressed exclusively in ADCs and SCCs, respectively. CK7 was both highly sensitive (95%) and specific (91%) for ADC. However, CK7 was less specific (72%) in PD ADCs. Desmocollin-3 was both highly sensitive (91%) and specific (100%). However, desmocollin-3 was not sensitive (59%) in PD SCCs.
AUC on ROC represents an optimal summary statistic for comparing the sensitivity and specificity of the markers. For 110 ADCs including all histologic grades, CK7 (0.97) had the greatest AUC, followed by napsin A (0.90), and TTF-1 (0.84). For 171 SCCs including all histologic grades, p63 (0.97) had the greatest AUC, followed by desmocollin-3 (0.96), CK5/6, and HMWCK (0.79). Analyzing 32 PD ADCs and 29 PD SCCs, p63 (0.95) had the greatest AUC, followed by napsin A (0.83), CK7 (0.83), CK5/6 (0.82), desmocollin-3 (0.79), TTF-1 (0.78), and HMWCK (0.77).
3) Sensitivity, specificity, PPV, NPV, and AUC on ROC of individual and combined markers in 32 PD ADCs and 29 PD SCCs
The sensitivities, specificities, PPV, NPV, and AUC on ROC of combined markers for PD ADC and PD SCC are presented in Tables 5 and 6, respectively. These findings indicate that the best single marker for PD ADC and PD SCC, based on sensitivity, specificity, and AUC on ROC, would be napsin A and p63, respectively. A combination of TTF-1 and napsin A increased the sensitivity (81%) and AUC on ROC (0.89) for PD ADC. However, desmocollin-3 and CK5/6 combined with p63 were not superior to p63 alone for PD SCC.
4) Immunohistochemical co-expression patterns of 32 PD ADCs and 29 PD SCCs
Immunohistochemical coexpression patterns for diagnosis of 32 PD ADCs and 29 PD SCCs were provided in Table 7. Since the reactivity for individual makers did not discriminate between ADC and SCC, we examined whether there was an overlap in expression for a various combination of markers. Eight Napsin positive cases were negative for TTF-1. Four TTF-1 positive cases were negative for napsin A. Double-negative profiles of TTF-1/desmocollin-3, napsin A/desmocollin-3, TTF-1/p63, napsin A/p63 were 43% (26/61), 34% (21/61), 23% (14/61), and 11% (7/61), respectively. On an Immunohistochemical basis, we could predict tumor subtypes in 52 of 62 PD NSCLC cases. In the negative expression of ADC markers (TTF-1 and napsin A) and SCC markers (p63 and desmocollin-3), 3 cases of PD ADCs were subtyped after mucicarmine staining. Both expression and/or no expression of ADC (TTF-1 and napsin A) and SCC markers (p63 and desmocollin-3) were diagnosed as NSCLC-NOS (10%, 6/61). Six NSCLC-NOS were 4 ADCs and 2 SCCs in reference diagnosis (diagnosis of resection specimen).
5) Panels of immunohistochemical and histochemical markers, and AUC on ROC using logistic regression analysis for subtyping 61 PD NSCLCs
Logistic regression analysis (Table 8) revealed that the combination of TTF-1, desmocollin-3, napsin A, and p63 was the best immunohistochemical marker panel for differentiating between ADC and SCC (0.995 AUC on ROC). In addition, mucin stain (e.g., mucicarmine) increased the AUC on ROC (0.997) and the cumulative accuracy of diagnosis improved to 90%.
DISCUSSION AND CONCLUSION
Histopathologic classification of lung carcinoma is important, as a prognostic factor and in the evaluation for potential treatment modalities. Although the reproducibility rate of the pathologic diagnoses, based on routine light microscopic features is satisfactory for distinguishing between SCLC from NSCLC and for detection of glandular vs. squamous differentiation in well to moderately differentiated ADC and SCC, it is less than satisfactory for identifying PD SCC from PD ADC, especially in small biopsy tissues obtained by bronchoscopy or gun biopsy. In addition, the distinction of PD NSCLC can be difficult in small tissue biopsies, due to a variety of factors, such as crush artifact, necrosis, less than optimal fixation, and the overlapping cytologic characteristics of these tumors. According to existing evidence, about 75% of NSCLCs in biopsies need only routine H&E staining to be identified as ADC or SCC (7,22). In our study, well to moderately-differentiated NSCLC (H&E stain-diagnosable) was 78%.
TTF-1 is a tissue-specific transcription factor that mediates cell determination and differentiation in lung, thyroid, and brain. It is normally expressed in alveolar pneumocytes, Clara cells, ciliated respiratory epithelial cells, and basal cells of the lung (23). TTF-1 positivity has been reported in 5 to 21% of SCCs (24-26). However, based on our study and that of others, TTF-1 does not stain pulmonary SCC (27-29). Napsin A, an aspartic proteinase involved in the maturation of surfactant protein B, has been favored as a new diagnostic marker for pulmonary ADC (12,30). As reported, it is normally expressed by type II pneumocytes, alveolar macrophages, and the epithelium of proximal and convoluted renal tubules (31). In a recent study, the sensitivities of TTF-1 and napsin A for pulmonary ADC were 73% and 83%, respectively (32). From our data, the sensitivities of TTF-1 and napsin A were 56% and 69% in PD ADC, respectively. Despite these lower figures in PD ADC, the sensitivity of napsin A was a higher than that of TTF-1. Eight Napsin positive cases were negative for TTF-1. Four TTF-1 positive cases were negative for napsin A (data not shown). Since TTF-1-postive/napsin A-negative or TTF-1-negative/napsin A-positive ADC does exist, combining the 2 markers (81% sensitivity) compared to napsin A alone (69% sensitivity) or TTF-1 alone (56% sensitivity) may have merit.
In the normal tissues, p63 was reported to be detectable by immunohistochemstry in basal cells of the squamous epithilia and basal cells of the bronchial epithelium. Furthermore, it is detectable in most SCCs of various primary sites, including SCC of the lung, and p63 positivity in pulmonary neoplasm is not limited to SCCs. Previous studies indicate that p63 may be the best marker for SCC, and our results showed that p63 was sensitive (97%) and specific (88%) for PD SCC. One large series of a TMA study of 408 cases of NSCLC showed that 30% of ADCs were p63 positive, while our results were 24% (26/110) (33). While expression of p63 was seen in a small proportion of non-SCC as well, especially in the ADCs, the intensity and the proportion of immunoreactive tumor cells were strong and diffuse with SCC and relatively weak and focal in ADC. The mean H score of PD SCC and PD ADC were 5.2 and 3.8, respectively. Different staining patterns can be helpful in this respect. In addition, we found that p63 was the best marker among SCC markers that could differentiate between pulmonary SCC and ADC, because p63 had the highest AUC on ROC irrespective of tumor differentiation. Desmocollin-3 is a protein found in desmosomes, and its expression was detected in 100% of pulmonary SCCs (18). Our study showed that desmocollin-3 was not expressed in ADC, irrespective of tumor differentiation, and had the highest specificity among the SCC markers tested. Desmocollin-3 expression in SCCs was influenced by tumor differentiation as p63. Monica and colleagues reported on the value of desmocollin-3 as a squamous cell marker, and TTF-1 in predicting the histologic type of 31 cytologic samples diagnosed as NSCLC-NOS (18). These 2 markers appear to be mutually expressed exclusively in ADCs and SCCs, respectively. The same result was also reached in our study. In our study, p63-postive/desmocollin-3-negative PD SCC was 10/29 (34%) and p63 was positive in all desmocollin-3 positive. Since desmocollin-3 was highly specific (100%) in PD SCC and p63 showed positivity in 4/32 (13%) in PD ADC, combination of the 2 markers may have merit to exclude the PD SCC. For example, if TTF-1 or napsin A is positive and p63 is positive, desmocollin-3-negative can exclude the diagnosis of SCC. However, desmocollin-3 had lower sensitivity (59%) compared to p63 (97%). A combination of the 2 markers (97% sensitivity) did not statistically increase the diagnostic performance compared to p63 alone (97% sensitivity). In addition, in 4 cases where p63 was positive in 32 PD ADC, the H score was lower than that of PD SCC (4 vs. 6 in mean). Also, the AUC on ROC used logistic regression analysis when looking at the combination of TTF-1, p63, and napsin A was the same (0.995) regardless of the existence or nonexistence of desmocollin-3. Thus, we excluded the desmocollin-3 from the immunohistochemical panel for subtyping PD NSCLC in our study.
The reported sensitivity of CK5/6 for pulmonary SCC ranges from 61% to 93% (16,17,22,29,34-36). Kargi et al. (16) found that p63 and CK5/6 differentially stained easily recognizable ADC and SCC with 89% specificity and 79% sensitivity. Kaufmann et al also found that combination of p63 and CK5/6 was superior to either marker alone in H&E stain-diagnosable, but the sensitivity diminished to 73% in PD SCC. Furthermore, they reported that if a positive result required >50% of cells to be stained, specificity rose to 99%, while sensitivity fell to 66% (34). In our study, CK5/6 had a lower sensitivity (76%) than p63 (97%) in PD SCC. The specificity was 88%, which was similar to p63. A combination of the 2 markers (100% sensitivity) slightly increased the diagnostic performance compared to p63 alone (97% sensitivity). However, the specificity decreased from 88% to 78%. In AUC on ROC analysis, CK5/6, p63, and the combination of the 2 markers were 0.82, 0.95, and 0.89, respectively. CK5/6 alone or combination was statistically superior to desmocollin-3 (0.79 AUC on ROC), but not to p63 which is in accordance with the results of a previous study (22,36). In our study, CK7 was both highly sensitive (95%) and specific (91%) for all grades of 110 ADCs. Even though,diffuse strong immunoreactivity was considered positive, CK7 was less specific (72%) in PD ADC. HMWCK for SCC was highly sensitive (95%) but too nonspecific (62%) to be diagnostically useful. In practice, ancillary immunohistochemical staining was needed in morphologically PD or undifferentiated carcinomas on routine H&E stain. Similar findings have been reported by other investigators, suggesting that CK7 and HMWCK should not be used to differentiate between ADC and SCC (13,37-39).
The usefulness of using multiple markers in clinical practice in helping to differentiate PD ADC from PD SCC is well established. The 2011 guidelines of the International Association for the Study of Lung Cancer (IASLC)/American Thoracic Society (ATS)/European Respiratory Society (ERS) for classification of lung ADC recommend that tissue allocated for stains of small biopsies be minimized (one SCC marker and one ADC marker or mucin stain) in order to preserve as much of the specimens as possible for molecular testing (40). The goal of some previous studies was to find the minimal number of markers needed for reliably subtyping PD NSCLC (22,29,36,39,41). Nicholson et al. proposed a panel of CK5/6, p63, TTF-1 and d-PAS stain during the biopsy and cytologic sample evaluation (39). Diagnostic refinement was enabled in 65% of tested questionable cases to either ADC or SCC. The study included CK5/6, HMWCK, p63, TTF-1 and d-PAS and did not include CK7, desmocllin-3 and napsin A in contrast to our study. Loo and colleagues successfully subtyped undifferentiated NSCLC in bronchial biopsy specimens using a mucin stain plus p63 and TTF-1 (22). This panel reduced the proportion of specimens labeled as NSCLC-NOS without definitive or probable histologic subtype to 7%. They studied markers including CK5/6, HMWCK, p63, S100A7, TTF-1 and mucin stain (alcian blue- periodic acid-Schiff). Because the scores for individual markers of CK5/6, HMWCK, and S100A7 could not be improved by considering combination scores for more than one marker, they excluded them in their study. Terry et al examined the expression of 9 markers (CK5/6, CK7, HMWCK, napsin A, NTRK1, NTRK2, p63, TTF-1, and mucicarmine) in TMA format, using logistic regression analysis and identified CK5/6, CK7, napsin A, p63, TTF-1 and mucicarmine as an optimal panel of markers (41). Mukhopadhyay and Katzenstein (29) further reported that a combination of CK5/6, napsin A, p63, and TTF-1 markers allowed accurate classification in 77% of PD NSCLCs (29). Noh and Shim (36) examined the expression of 6 markers (CK5/6, CK7, napsin A, p63, SOX2, and TTF-1) in TMA format and identified the panel of napsin A, p63 and TTF-1. In these previous studies, TTF-1 and napsin A served as a marker of ADC and p63 as a marker of SCC. In our study, PD NSCLC can be accurately subtyped on TMA simulating small biopsy conditions in 78% cases of PD ADCs and 93% of PD SCCs using a combination of TTF-1, p63 and napsin A. Mucin stains for PD NSCLCs increased the accuracy for diagnosing PD ADC (88%). Mucin stains, such as diastase-periodic acid-Schiff, alcian blue and mucicarmine, are helpful to increase the accuracy of diagnosis to differentiate NSCLC-NOS.
The 2011 IASLC/ATS/ERS guidelines discourage diagnosis of large cell carcinoma (LCC) from limited biopsies or by cytology (40). At present, LCC is a diagnosis of exclusion, to be made via surgical resection. LCC can be diagnosed if p63, TTF-1, desmocollin-3, and napsin A are all negative in the resected specimen. Since none of the markers studied are highly sensitive or specific for a particular tumor subtype, PD NSCLCs cannot be classified, even with immunohistochemical support, and are currently designated as 'NSCLC-NOS' in biopsy or cytology reporting, allowing patient eligibility for further molecular testing (40). Our data showed that 6 of 61 PD NSCLCs had a non-predictive immunophenotype. No SCC showed an ADC immunophenotype and vice versa. Both expression and/or no expression of ADC (TTF-1 and napsin A) and SCC markers (p63 and desmocollin-3) were diagnosed as NSCLC-NOS (10%, 6/61). Of the 6 NSCLC-NOS specimens, 4 were ADC and 2 were SCC in reference diagnosis (resection specimen).
In conclusion, we recommend a minimal panel of immunohistochemical and histochemical markers to include TTF-1, p63 napsin A and one of mucin stains for tumor subtyping of PD NSCLC in a small biopsy sample. This recommended panel reached an accuracy of 90% for subtyping PD NSCLC.







 XML Download
XML Download