

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
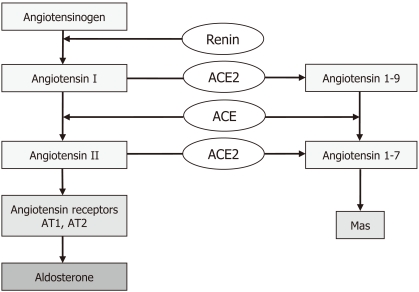
The renin-angiotensin system (RAS) is a pivotal mediator of renal and vascular homeostasis. Its systemic actions include the regulation of blood pressure, natriuresis, and blood volume control. The RAS also plays an important role at a local level, regulating regional blood flow and controlling trophic and fibrotic responses to a range of stimuli. The RAS is composed of a number of different regulatory components and effector molecules. Angiotensin II (Ang II) acts by binding to Ang II type 1 (AT1) and Ang II type 2 (AT2) receptors. The angiotensin-converting enzyme (ACE)-Ang II-AT1 receptor axis has important physiologic and pathologic roles. However, the recent discovery of ACE-related carboxypeptidase (ACE2) and angiotensin 1-7 (Ang-(1-7)) has changed the way in which the RAS is viewed (Fig. 1). Ang-(1-7) is present in the kidneys at concentrations comparable to those of Ang II and is associated with vasodilation, modulation of sodium and water transport, and stimulation of nitric oxide (NO) synthase1-3).
ACE2 and Ang-(1-7)
ACE2 is a type 1 integral membrane glycoprotein that is found in most tissues, with its highest expression observed in the kidneys, endothelium, and heart4, 5). The extracellular surface of the ACE2 enzyme contains a single catalytic metallopeptidase domain that shares 42% sequence identity and 61% sequence similarity with the N-terminal catalytic domain of somatic ACE. ACE2 is an exopeptidase that catalyzes the conversion of Ang I to the nonapeptide Ang-(1-9) and the conversion of Ang II to the heptapeptide Ang-(1-7). The primary role of ACE2 is converting Ang II into Ang-(1-7) with an efficacy > 400-fold greater than that of the hydrolytic action of ACE2 in forming Ang-(1-9)6). ACE2 is associated with a reduction in Ang II and an increase in Ang-(1-7) levels. ACE2 protein levels are significantly decreased in the kidneys of hypertensive patients, and patients with late diabetic nephropathy7, 8).
The heptapeptide Ang-(1-7), generated from either Ang I or Ang II, acts by opposing the vasoconstrictor, proliferative, and profibrotic actions of Ang II in the circulation and in cardiac, vascular, and renal tissues9, 10). In a type 2 diabetic animal model, Ang-(1-7) attenuated Ang II-mediated NAD(P)H oxidase activation and reactive oxygen species production in diabetic glomeruli and mesangial cells were noted11). Ang-(1-7) also binds to the Mas receptor, a seven transmembrane protein with domains containing sequences characteristic of G-protein coupled receptors. The Mas receptor is expressed in renal proximal tubular cells, afferent arterioles, cardiac myocytes, and neuronal cells. It conveys Ang-(1-7) signals via transcriptional factors.
Effects of ACEI and angiotensin II receptor blockers (ARBs) partly depend on ACE2 and Ang-(1-7)
ACE inhibitors and receptor blockers can affect the ACE2-Ang-(1-7) system. ACE inhibitors increase the production of Ang I, which is converted to Ang-(1-7) by ACE2, and endopeptidase. The antihypertensive actions of ACE inhibition are obtained by increased excretion of Ang-(1-7), which was observed in urine samples of patients with essential hypertension whose blood pressure was controlled by 6 months of treatment with captopril12). Blockade of AT1 receptors may be particularly important because the increase in the concentration of Ang II will stimulate greater production of Ang-(1-7). In addition, the low affinity binding of Ang-(1-7) to the AT1 receptor may allow the peptide to act as an antagonist in the presence of Ang II. ARB and olmesartan-treated spontaneously hypertensive rats (SHR) showed upregulation of ACE2 mRNA in the aorta as well as plasma Ang-(1-7) levels, which was related to the selective reduction of the thoracic aorta media-to-lumen ratio and media thickness associated with olmesartan13).
The ACE2-Ang-(1-7)-Mas receptor axis in hypertension: focus on the kidneys
Numerous studies have documented the presence of RAS components in the kidneys, indicating that the kidney is a site at which an intrarenal system participates in the regulation of glomerular-tubular balance. ACE and ACE2 are expressed in the renal proximal tubules, but inside the glomeruli, they are mainly expressed in the podocytes14). In normal kidneys, high constitutive levels of ACE2 and a higher ACE2/ACE ratio may be associated with an increase in the Ang II breakdown system compared to Ang II generation, which may be important for maintaining the normal physiological and biological effects of Ang II. In contrast, increased ACE and decreased ACE2 with a higher ACE/ACE2 ratio in hypertensive kidneys may favor Ang II generation, leading to hypertensive cardiovascular and renal damage15). Elevated Ang II induces ACE expression and downregulates ACE2 expression by HK-2 cells. Increased expression of cortical and medullary Ang II and cortical ACE2 activity was also found in a model of hypertension with increased tissue renin. In an experimental model of renal hypertension, the administration of a selective Ang-(1-7) receptor blocker or an ACE2 inhibitor was associated with worsening of hypertension and renal function16). Ang-(1-7)-mediated increases in renal blood flow was abolished by blockade of the Mas receptor and by inhibition of prostaglandin release and nitric oxide in SHR and Wistar-Kyoto (WKY) controls3, 17, 18).
The systemic vasodilator effects of Ang-(1-7) are not consistently observed in animals with an intact baroreceptor reflex, or in conditions where there is no activation of the endogenous RAS. In a type 2 diabetic animal model, exclusive Ang-(1-7) infusion did not result in any changes in blood pressure or microalbuminuria. Likewise, ACE2-knockout mice showed mild elevation of blood pressure, but renal injury was minor. However, after acute Ang II infusion, plasma concentrations of Ang II increased and were almost 3-fold higher in ACE2-deficient mice than in controls. In a model of Ang II-dependent hypertension, blood pressure was substantially higher in ACE2-deficient mice compared with wild-type mice. The vascular response to Ang-(1-7) (and, by association, ACE2) was augmented in the following conditions: low salt diet; renin transgenic hypertensive rats; and Ang II infusion. In all of these conditions, endogenous RAS was stimulated.
Sexual differences in blood pressure related to the ACE2-Ang-(1-7)-Mas axis
Male SHR have elevated blood pressure and a higher incidence of albuminuria compared to age-matched female SHR19, 20). Treatment of male and female SHR with enalapril reduced blood pressure to similar levels in both sexes, indicating that both hypertension and sex differences in blood pressure are RAS mediated21). There are known sex differences in the expression levels of RAS components, and in functional responses to Ang II infusion. Young male SHR have higher levels of AT1 mRNA and protein expression in the kidneys, aorta, and mesenteric arteries, while AT2 mRNA expression is higher in females22). Sullivan et al. reported that Ang-(1-7) levels were greater in female compared with male SHR under basal conditions as well as following Ang II infusion, but Ang-(1-7) receptor antagonism abolished the sex differences in blood pressure response to Ang II infusion23). In this study, A-779 resulted in an initial increase in blood pressure sensitivity to Ang II and in proteinuria, especially in females, suggesting that Ang-(1-7) antagonizes immediate Ang II-induced increases in blood pressure and renal injury.
Conclusions
ACE2 is a functional component of the RAS; ACE2 metabolizes Ang II and produces Ang-(1-7), thereby contributing to regulation of blood pressure and progression of renal disease.
Effects of ACEI and ARB partly depend on ACE2 activation.
The vascular response to Ang-(1-7) (and by association, ACE2) is augmented in conditions where the endogenous RAS has been stimulated.
Sexual differences in blood pressure are associated with the ACE2-Ang-(1-7)-Mas receptor axis.
Targeting the ACE2-Ang-(1-7)-Mas receptor axis may be a novel therapeutic strategy for hypertension and diabetic kidney disease.
 XML Download
XML Download