

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Vitamin D is known to be essential for bone metabolism. The number of peer-reviewed publications with the term 'vitamin D' in their title or abstract has increased greatly since the early 2000s1). PubMed currently lists over 25,000 publications from 1950 to the present. In the 1960s, fewer than 100 papers on 'vitamin D' were published per year; however, in 2010, this rate of publication reached approximately 2,500 papers per year. This expansion of research over recent decades has resulted in a dramatic increase in our understanding of additional biological actions of vitamin D on various systems including pancreas β-cell function, immune, cardiovascular, muscle, and brain systems, and control of the cell cycle. An interesting relationship exists between mortality in ischemic heart disease and geographic latitude in European countries2), which shows an increase in the mortality of heart diseases with increase in latitude. Additionally, serum 25-hydroxyvitamin D (25(OH)D) levels have been shown to be higher in healthy subjects at lower latitudes2).
Go to : 
Vitamin D, hyperparathyroidism, and vascular calcification
Vitamin D plays a well-known role in the regulation of phosphate homeostasis. Phosphate is absorbed from the diet in the gut, stored in the skeleton, and excreted by the kidneys; 1,25-dihydroxyvitamin D (1,25(OH)2D) stimulates absorption of phosphate from the diet3). Fibroblast growth factor (FGF)-23 increases renal phosphate clearance, suppresses synthesis of 1,25(OH)2D, and may decrease parathyroid hormone (PTH). PTH increases renal phosphate clearance and stimulates synthesis of 1,25(OH)2D4). In chronic kidney disease (CKD) patients, ionizing calcium (iCa) is decreased secondary to phosphate retention and decrease in 1,25(OH)2D. Phosphate retention increases FGF-23, which, in conjunction with its cofactor, Klotho protein, decreases the activity of 1α-hydroxylase and increases 24α-hydroxylase, thus decreasing the levels of circulating 1,25(OH)2D. Additionally, phosphate retention results in an increase in posttranscriptional synthesis of PTH. Decreases in the vitamin D receptor (VDR), calcium sensor receptor, and Klotho-FGFR1 receptor complex in the parathyroid gland aggravate the development of the secondary hyperparathyroidism in CKD patients4).
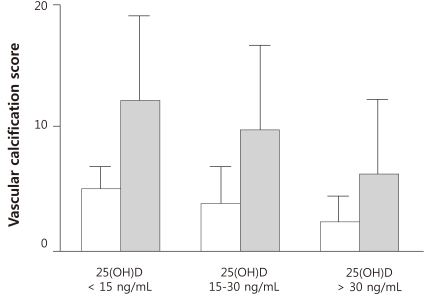
Apart from hyperparathyroidism, calcium and phosphate imbalance and vitamin D deficiency also contribute to vascular calcification. A cross-sectional study by Gracia-Canton et al. has reported an independent negative association between serum levels of 25(OH)D and vascular calcification in 210 patients with stage 4 and 5 CKD5). Plain X-ray images of pelvis, hands, and lateral lumbar spines from all subjects were studied for calculation of semi-quantitative vascular calcification scores, as described by Adragao6) and Kauppila7). Adragao scores revealed only 47 patients (22.4%) without vascular calcification and 120 patients (57.1%) with scores higher than 35). Kauppila scores revealed only 29 patients (13.8%) without aortic calcifications and 114 patients (54.3%) with scores higher than 75). Higher vascular calcification scores were related to older age, diabetes, history of cardiovascular disease (CVD), and lower levels of 25(OH)D5). Only one-fifth of patients had adequate levels of 25(OH)D, whereas a half had vitamin D insufficiency, and a quarter had vitamin deficiency (Fig. 1)5).
Go to :
Vitamin D and vitamin D receptor
Vitamin D is a multifunctional hormone that can affect many essential biological functions, ranging from immune regulation to mineral ion metabolism. Calcitriol or 1,25(OH)2D is the active form of vitamin D, formed by dual hydroxylation in the liver and kidney. Figure 2 shows a simplified diagram of the different stages of vitamin D synthesis8). Vitamin D2 (ergocalciferol), which is absorbed mainly from food, and vitamin D3 (cholecalciferol), produced in the skin by photolytic cleavage of 7-dehydrocholesterol, is transported to the liver and converted to 25(OH)D, the major circulating metabolite of vitamin D. The final activation step, 1-hydroxylation, occurs primarily, but not exclusively, in the kidney, forming 1,25(OH)2D8).
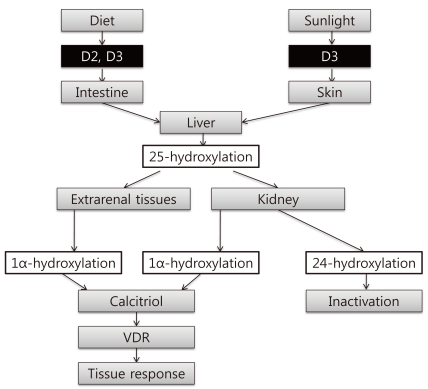 | Fig. 2Synthesis of Vitamin D. D2, vitamin D2; D3, vitamin D3; VDR, vitamin D receptor.
*Modified from the study of Razzaque MS. Ref. 8.
|
Active vitamin D metabolites exert biological activities mainly through the VDR1). VDRs are operational in at least 38 tissues of the body. In these target tissues, VDR functions in the cell nucleus as a transcriptional factor influencing approximately 3% of the human genome, and in the plasma membrane caveolae as a modulator of signal transduction pathways (Fig. 3). The activity of the VDR conformational ensemble (with 2 ligand pockets) can generate either genomic or rapid biological responses. In this model, one shape (6-s-trans) of the conformationally flexible 1α,25(OH)2D can interact with VDR localized in the cell nucleus to generate genomic responses via regulation of gene transcription, whereas a different shape (6-s-cis) of 1α-25(OH)2D binds to the second ligand pocket of the VDR associated with caveolae of the plasma membrane to generate rapid responses1). VDR activation through these pathways has been shown to have wide-ranging effects. Calciotropic functions of 1,25(OH)2D include physiological regulation of calcium transport and bone mineralization. Synthesis of circulating 1,25(OH)2D, which mediates these calciotropic actions, is tightly regulated. Non-calciotropic actions involve activation of VDRs by locally produced 1,25(OH)2D in a number of tissues in a paracrine and autocrine fashion9). In particular, vitamin D is closely linked to CVD2). Experimental studies have shown that vitamin D treatment reduces neurohormonal activation, inhibits inflammation, and suppresses ventricular hypertrophy10).
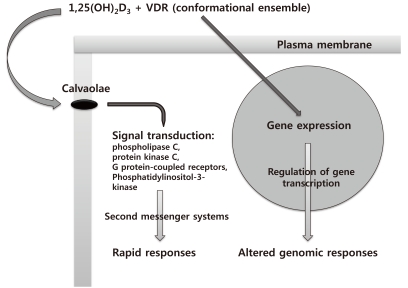 | Fig. 3Function of Vitamin D Receptor (VDR) Conformational Ensemble: Genomic or Rapid Responses.
*Modified from the study of Norman AW et al. Ref. 1.
|
Go to :
Vitamin D deficiency in CKD
The recent Workshop Consensus for Vitamin D Nutritional Guidelines estimated that approximately 50% and 60% of the older populations in North America and the rest of the world, respectively, do not have satisfactory vitamin D status11). The consensus further concluded that the situation is similar in younger subjects. Reasons for this remain unclear but are probably related to factors such as urbanization, demographic shifts, decreased outdoor activity, air pollution, global dimming, and decrease in cutaneous production of vitamin D with age. Epidemiological investigations in many countries have shown high prevalence of unsatisfactory vitamin D status (Table 1)12-15). In particular, the 2008 Korea National Health and Nutrition Examination Survey (KNHANES) found vitamin D insufficiency in 47.3% of male and 64.5% of female subjects15).

The outpatient cross-sectional cohort study conducted by Levin et al. has revealed that abnormalities of mineral metabolism occur early in CKD16). A decrease in 1,25(OH)2D levels was above the range of glomerular filtration rate (GFR) values even in the early stage of CKD16). Similarly, significant inverse correlations were observed among serum phosphate, FGF-23 and PTH levels, and GFR in patients with stage 1 to 3 CKD17). Hypovitaminosis D is prevalent even in patients with early-stage CKD18). It is consistent with the previous data that 25(OH)D deficiency worsens with the progression of CKD. Therefore, the Kidney Disease: Improving Global Outcomes (KDIGO) Clinical Practice Guidelines have recommended annual measurement of 25(OH)D and have also recommended that the level should be maintained at 30 ng/mL or higher in patients with any stage of CKD19).
Go to :
Decreased VDR activation and clinical outcomes
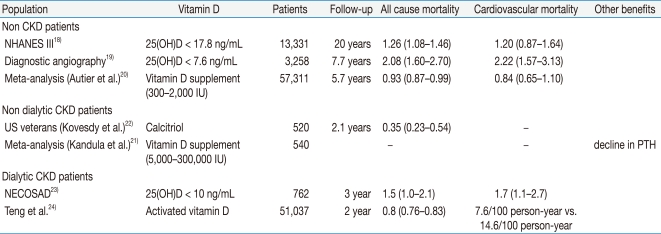
Melamed et al. tested the association of low 25(OH)D levels with all-cause, cancer, and CVD mortality in 13,331 nationally representative adults from the Third National Health and Nutrition Examination Survey (NHANES III) linked mortality files20). In this cross-sectional multivariate analysis, increasing age, female sex, non-white race/ethnicity, diabetes, current smoking, and higher body mass index were all independently associated with higher odds of 25(OH)D deficiency, whereas greater physical activity, vitamin D supplementation, and non-winter season showed an inverse association20). In multivariate models, compared with the highest quartile, being in the lowest quartile for 25[OH]D levels (< 17.8 ng/mL) was associated with a 26% increased rate of all-cause mortality (mortality rate ratio, 1.26; 95% CI, 1.08-1.46) and a population attributable risk of 3.1%20). The prospective cohort study by Dobnig et al., which enrolled patients undergoing diagnostic coronary angiography with normal kidney function showed a similar result with regard to relationships between endogenous 25(OH)D and 1,25(OH)2D levels and all-cause and cardiovascular mortality21). Multivariate-adjusted hazard ratios (HRs) for patients with lower levels of 25(OH)D were two times higher for all-cause mortality and cardiovascular mortality21).
A meta-analysis of randomized controlled trials by Autier and Gandini showed that intake of ordinary doses of vitamin D supplements appears to be associated with decreases in total mortality rates22). They have identified 18 independent randomized controlled trials, including 57,311 participants. The relative risk for mortality from any cause was 0.93 (95% CI, 0.87-0.99)22). Kandula et al. have reported on vitamin D supplementation in CKD by meta-analysis23). Among observational studies and randomized controlled trials, significant improvement was observed in serum 25(OH)D levels, along with an associated decline in PTH levels23). A low incidence of hypercalcemia and hyperphosphatemia has been reported with vitamin D supplementation. However, included studies were mostly of low to moderate quality and did not show beneficial effects on hard clinical endpoints23). Kovesdy et al. reported on the benefit of activated vitamin D treatment in patients with predialysis CKD24). Two hundred fifty-eight of 520 subjects received treatment with calcitriol. The incidence rate for mortality and combined death and dialysis initiation was significantly lower in treated than in untreated patients. Treatment with calcitriol was associated with a trend toward a lower incidence of dialysis. These results were consistent across different subgroups24).
One prospective cohort study of incident dialysis patients in the Netherlands (the NECOSAD) revealed an association of vitamin D deficiency in dialysis patients with an adverse health outcome, in particular, with short-term cardiovascular mortality25). Teng et al. reported on a historical cohort study of activated injectable vitamin D and hemodialysis survival26). During a 2-year observational period, 37,173 patients on hemodialysis received activated injectable vitamin D, and 13,864 did not. At 2 years, the mortality rate was 13.8/100 person-years in the group that received injectable vitamin D, compared with 28.6/100 person-years in the non-vitamin D group (P < 0.001). The incidence of cardiovascular-related mortality was 7.6/100 person-years in the injectable vitamin D group, compared with 14.6/100 person-years in the non-vitamin D group (P < 0.001). The study by Wolf et al. also showed that, although low vitamin D levels were associated with increased mortality, significant interactions were noted among vitamin D levels, subsequent active vitamin D therapy, and survival27). Compared with patients with the highest 25(OH)D or 1,25(OH)2D levels who received therapy, untreated deficient patients showed a significantly increased risk for early mortality27) (Table 2).
Go to :
Summary
In summary, vitamin D deficiency is common not only in CKD patient but also in the general population. Reduced VDR activation occurs early in CKD. Low 25(OH)D is a risk factor for and is predictive of cardiovascular events. Decreased VDR activation is a major pathophysiological factor in the development of secondary hyperparathyroidism and also contributes to CKD morbidity and mortality. Patients with CKD have reduced VDR activation. Restoration of the physiology of VDR activation should be essential therapy for CKD patients.
Go to :
 XML Download
XML Download