

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Acute diarrhea is a major problem worldwide, although the overall mortality rate from diarrheal disease has steadily declined over the last few decade1). The critical factor for the reduction in the mortality from diarrhea was the introduction of oral rehydration therapy (ORT). The standard World Health Organization oral rehydration solution (WHO-ORS) was initially assessed for cholera treatment, and then shown to be effective irrespective of cause of diarrhea or age of the patient2). However, the WHO-ORS does not substantially decrease either stool volume or the duration of diarrhea episodes3). As a result, improved ORSs for enhancing treatment of acute diarrhea continually have been sought for and evaluated.
Go to : 
Pathophysiologic basis for using ORS
In an adult, the daily intestinal water load is approximately 6,500 mL from the combination of oral intake, gastric juices and pancreaticobiliary juices, as well as an additional 1,000 mL secreted by the upper intestine. This volume is reduced to 1,500 mL by the distal ileum and is further reduced in the colon to a stool output of 250 mL per day4). The net absorption of water and ions is the result of two opposing unidirectional fluxes of ions, one absorptive and the other secretory. And the two processes are anatomically separated: absorption takes place mainly in the mature villous cells, whereas secretion seems to occur in the crypt cells5). In normal circumstances, absorptive processes for water and electrolytes prevail over secretory processes and as a result, water is absorbed. However, during diarrheal disease, there is a derangement in the absorptive-secretory processes by osmotic and/or secretory mechanisms. The absorption of water and nutrients is dependent on the osmotic gradient dictated by sodium transport via the following three mechanisms: neutral NaCl absorption, sodium absorption coupled to the absorption of organic solutes such as glucose and amino acids, and electrogenic sodium absorption5). In diarrheal disease, disruption of these processes occurs except the sodium absorption coupled glucose and other organic solutes, even in enteritis associated with epithelial damage6, 7). The preservation of this facilitated cotransporter of glucose and sodium is the scientific rationale for the development of the ORS. By this intact Na+/glucose cotransporter, unaffected by pathologic processes that induce secretion, sodium and water are absorbed and in turn, extracellular fluid is expanded without change in serum osmolarity8).
Go to :
Efficacy of ORS
ORS has several advantages compared with intravenous fluid therapy (IVT). It is convenient to administrate and does not accompany pain or phlebitis. Moreover, based on the results of meta-analyses of randomized controlled studies9, 10), the effectiveness of the ORS has been shown to be similar with intravenous rehydration for treating acute gastroenteritis in children. There was no difference in the frequency of stool, duration of diarrhea, weight gain or development of hypo or hypernatremia between the ORS group and the IVT group. In addition, there was a shorter hospital stay in the ORS group. However, paralytic ileus occurred more frequently in the ORS group. According to these results, the ORT has advantages in all aspects except the development of paralytic ileus compared with IVT.
Go to :
Standard WHO-ORS
In 1975, the WHO first introduced an ORS that subsequently has been used throughout the world for more than 25 years. This ORS was initially designed to treat children with diarrhea from cholera. The standard WHO-ORS has an osmolarity of 311 mOsm/L and concentrations of sodium at 90 mEq/L, potassium at 20 mEq/L, chloride at 80 mEq/L and glucose at 20 g/L11). However, subsequently, it became clear that the composition of the standard WHO-ORS could not be optimized to help reduce the volume of stool and duration of diarrhea, although hydrational status could be maintained3). The concentration of sodium was too high for well-nourished children with noncholeral diarrhea12). This has led to a search for an ORS with improved compositions.
Go to :
Reduced osmolarity ORS
Animal studies13) and in vivo human intestinal studies14) have shown that reduced osmolarity ORS resulted in increased water absorption when compared with the standard ORS in acute non-cholera diarrhea. Similar observations have been reported in human studies15, 16). In a meta-analysis by Hahn et al.17), the effectiveness and complications of reduced-osmolarity ORS (osmolarity less than 250 mOsm/L) was compared with those of the standard WHO-ORS in 2,397 patients with acute diarrhea of less than 5 days duration. This study included 12 trials of non-cholera patients and 3 of cholera patients. They concluded that there were reductions in stool output, episodes of vomiting and the need for intravenous hydration in the reduced-osmolarity ORS group. Furthermore, on the basis of the results in 6 trials measuring serum sodium values with events in 3 studies, the incidence of hyponatremia was not different between both groups18). According to this finding, the WHO changed its recommendations for acute non-cholera diarrhea in children; the composition of the ORS to a lower osmolarity (245 mOsm/L) and to lower concentrations of glucose (13.5 g/L) and sodium (75 mEq/L)19).
However, the optimal osmolarity is still debated, especially in adult patients with cholera5). Although there was no additional risk of hyponatremia in children receiving the reduced osmolarity ORS18), further trials in adults with cholera may be necessary if a single ORS formulation is to be used for cholera and noncholera patients5).
Go to :
Polymer-based ORS
The substitution of glucose monomer in the ORS with glucose polymers such as whole rice and wheat has been evaluated as a method to decrease both the volume and duration of diarrhea20, 21). The aim for this is to slowly release glucose into the gut and improve the absorption of water and salt in the solution22, 23). A recently published meta-analysis by Gregorio et al.24) compared polymer-based ORS with glucose-based ORS for treating acute watery diarrhea. This study included 34 trials involving 4,214 participants with diarrhea (27 trials in children, 5 in adults and 2 in both) and most compared polymer-based ORS with high-osmolarity ORS (more than 310 mOsm/L). They concluded that polymer-based ORS was judged superior to the WHO-ORS in the treatment of diarrhea of all causes overall, and specifically in the treatment of cholera-induced diarrhea, in terms of fewer unscheduled intravenous infusions and shortened diarrhea duration. However, the analysis was underpowered to favor polymer-based ORS over reduced osmolarity ORS, and further trials against the current standard (ORS with osmolarity less than 250 mOsm/L) are required.
Go to :
Zinc supplementation
Diarrhea can lead to zinc deficiency, and the resulting zinc deficiency can lead to a vicious cycle of worsening duration and severity of diarrhea25). The beneficial effects of zinc include improved cellular immunity and maintenance of gut mucosal cells26). The effectiveness of zinc for treating diarrhea has been evaluated in several studies27-29). Baqui AH et al.29) reported a 24% reduction in diarrhea-related hospitalization rate and overall decrease in mortality. In a meta-analysis of 16 trials that included 15,231 participants with acute diarrhea and 6 trials that included 2,968 participants with persistent diarrhea30), zinc supplementation resulted in a reduction of the mean duration of both acute and persistent diarrhea as well as a reduction in stool frequency. However, its supplementation was associated with a greater incidence of vomiting in 11 of the acute diarrhea trials and in 4 persistent diarrheal trials30). Based on the proven safety and effectiveness of zinc supplementation as an adjunct therapy for diarrhea, the WHO recommends oral zinc for 10-14 days at 20 mg per day in children older than 6 months and 10 mg per day in children younger than 6 months for acute diarrheal illness19). There are no specific recommendations for zinc supplementation for adults because of a paucity of data from adults, although the mechanism of action would presumably be the same19).
Go to :
Commercial ORS
Commercially available ORS vary in osmolarity and sodium concentration (Table 1). Studies in the United States showed that children with mild to moderate dehydration were treated successfully with commonly used commercial ORS31, 32). In children between 5 and 10 years of age, sucralose-sweetened ORSs (for example, Pedialyte and Pediatric Electrolyte) appear to be more palatable than comparable rice-based solutions such as Enfalyte33). Other nonphysiologic fluids such as sports drinks and soft drinks have too little sodium and much higher osmolarity than recommended. These fluids are not suitable for diarrheal treatment as they may cause osmotic diarrhea and hyponatremia (Table 1).
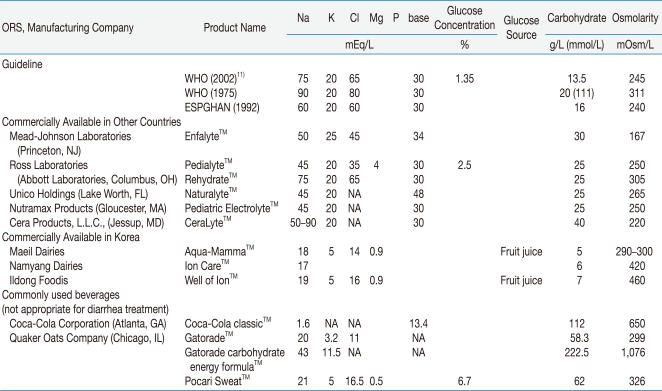
Table 1
Composition of Commercial Oral Rehydration Solutions (ORS) and Commonly Consumed Beverages
NA, not applicable; WHO, World Health Organization; ESPGHAN, European Society for Paediatric Gastroenterology, Hepatology and Nutririon.
*Modified from the previous study of Atia AN et al. Ref.19.
![]()
Go to :
Conclusion
ORS has been used successfully in the treatment of diarrheal illness and has resulted in a reduction in childhood mortality from diarrhea. The standard WHO-ORS has been used to replace water and electrolytes lost in stools, but it does not decrease diarrhea duration or the stool volume. This has led to search for modified ORSs with improved efficacy. Reduced osmolarity ORS is superior in that it has been found to decrease the fecal volume and duration of diarrhea. Because of that, it is currently used as a recommended ORS formulation by the WHO for the treatment of acute non-cholera diarrhea. The addition of zinc supplementation is recommended by WHO in the treatment of acute diarrhea. Polymer-based ORS seems to be superior than the standard WHO-ORS for treating acute diarrhea, but further studies against the current reduced osmolarity ORS are needed.
Go to :
 XML Download
XML Download