

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Renal function and blood pressure are tightly linked and hypertension per se is a risk factor for the development of end-stage renal disease (ESRD)1, 2). The renin-angioten-sin-aldosterone system (RAAS) is a key regulator of both blood pressure and renal function, so that genes encoding components of the RAAS can be candidate genes for evaluating predisposition for the development of hypertension, cardiovascular disease and progression of renal disease. Polymorphisms have been described in the genes encoding several important components of the RAAS, including angiotensinogen3), angiotensin-converting enzyme4), angiotensin type I receptors5), and aldosterone synthase6).
The aldosterone synthase gene, CYP11B2, encodes for a cytochrome P450 enzyme, involved in the terminal steps of aldosterone synthesis in the zona glomerulosa cells of human adrenal glands and its expression is regulated by angiotensin II and potassium7). The CYP11B2 -344C/T polymorphism, which is located at a putative binding site for the steroidogenic transcription factor (SF-1), has been reported to be associated with serum aldosterone level8), urinary aldosterone excretion9), blood pressure9-12), left ventricular size and mass13, 14). However, there were few studies on the association of CYP11B2 -344C/T polymorphism and renal function, which has inconsistent results15, 16). The aim of this study is to evaluate the relation between CYP11B2 polymorphism and ESRD in the Korean population and the association with CYP11B2 polymorphism and cardiovascular morbidity in ESRD patients on hemodialysis.
Go to : 
Methods
1. Subjects
The study subjects were 271 ESRD patients on maintenance hemodialysis over three months from dialysis centers located in the western district of Seoul, Korea and 134 control subjects without renal disease from Korea University Guro Hospital. The controls were individuals who have had no medical history and were normal in blood pressure, blood chemistry, urinalysis, and electrocardiogram (EKG).
Basic demographic data, current blood pressure, information on underlying renal disease, previous cardiovascular disease, and current antihypertensive medication were obtained for all ESRD subjects. Left ventricular hypertrophy was determined as the voltage sum SV1+ (RV5 or RV6) ≥35 mm using the Sokolow-Lyon voltage criteria on EKG17). Clinical cardiovascular diseases include ischemic heart disease, cerebrovascular disease and congestive heart failure. Ischemic heart disease was considered if the patient had previous myocardial infarction, positive coronary angioplasty or other diagnostic procedure (e.g. exercise test, thallium or dobutamine stress test) or the presence of ischemic change on the resting EKG (as distinct from left ventricular hypertrophy). Cerebrovascular disease was established if the patient had a history of transient ischemic attacks or stroke verified by computed tomography, or carotid artery stenosis greater than 70% verified by doppler ultrasound. Congestive heart failure was defined as clinical evidence of pulmonary edema, not attributable to errors in fluid balance, and/or moderate to severe left ventricular dysfunction on echocardiography (left ventricular ejection fraction <45%). In addition, biochemical data including plasma hemoglobin, hematocrit, serum albumin, creatinine, glucose, total cholesterol, total calcium, phosphorus, intact parathyroid hormone, and single-pool Kt/V were obtained.
2. Genotyping
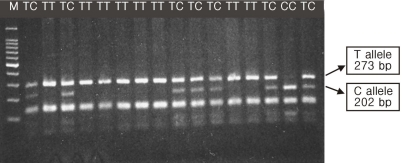
Genomic DNA was extracted from peripheral blood using the DNA extraction kit (G-DexTM IIb No.17241, iNtRON). Genotypes were determined by polymerase chain reaction (PCR) amplification of the promoter region of the CYP11B2 gene using the oligonucleotide primers (upstream: 5'-CAG GAGGAGACCCCATGTGAC-3'; downstream: 5'-CCTCC ACCCTGTTCAGCCC-3'). PCR conditions were: initial denaturation at 94℃ for 3 min; then 32 cycles at 94℃ for 1 min, at 60℃ (annealing) for 1 min, and at 72℃ (extension) for 1 min. Restriction fragment length polymorphism (RFLP) was performed by adding 10 U of restriction endonuclease HaeIII site in the appropriated buffer to 5 µL from each reaction (a 537 bp product) and by incubating at 37℃ for 2 hours. The samples digested then underwent electrophoresis on 2.5% agarose gel with a Gel Electrophoresis Apparatus, ethidium bromide stained, and analyzed under UV lights. Since the (-344)T allele lacks an HaeIII site (GGCC) present in the (-344)C allele, the (-344)T alleles are detected as fragments of 273 bp and (-344)C alleles as fragments of 202 bp (plus smaller fragment in each case) (Fig. 1).
3. Statistical analysis
Statistical analysis was performed using the Statistical Package for Social Sciences (SPSS-12.0, Chicago, Illinois, USA). Values are expressed as mean±standard deviation (SD) or percentage. Statistical differences between means were assessed by t test or analysis of variance (ANOVA) for analysis of continuous variables. For categorical variables, the 2×2 contingency table χ2 test was used. To examine the independent contribution of CYP11B2 polymorphism and estimate the odds ratio, while adjusting for the effects of other clinical characteristics, we used a logistic analysis. The Hardy-Weinberg equilibrium was tested by a χ2 test. P values below 0.05 were considered statistically significant.
Go to :
Results
The baseline characteristics of controls and ESRD patients are summarized in Table 1. The mean age and male prevalence were similar between controls and ESRD patients. Genotype and allele frequencies for the polymorphism of CYP11B2 in controls and ESRD patients are presented in Table 2. The controls and ESRD patients were in Hardy-Weinberg equilibrium for the polymorphism. Genotype distribution of CYP11B2 polymorphism did not differ between controls and ESRD patients.
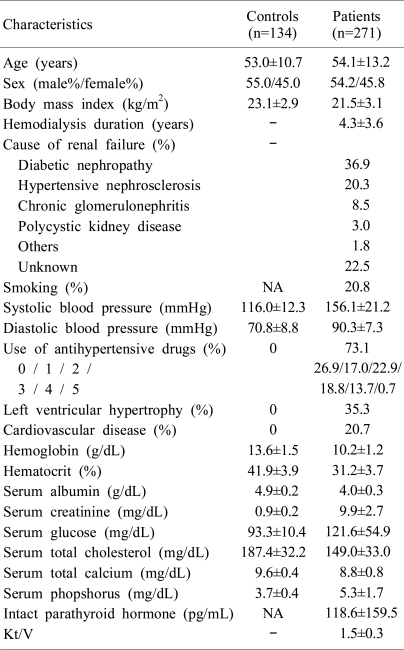
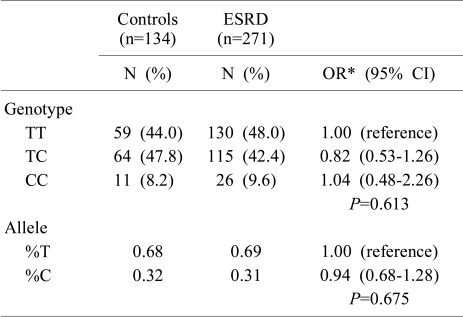
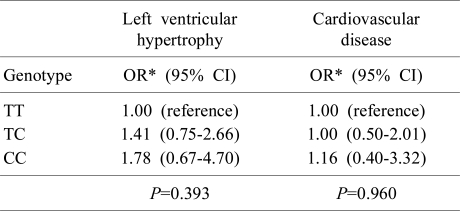
Table 3 shows the comparison of clinical and biochemical characteristics of ESRD patients according to genotypes of CYP11B2 polymorphism. We could observe the differences in systolic blood pressure and frequency of diabetes among the three genotypes in this analysis. However, these findings were not significant after adjustment for age and sex. In addition, there was no association of CYP11B2 polymorphism with left ventricular hypertrophy or cardiovascular disease in ESRD patients (Table 4).
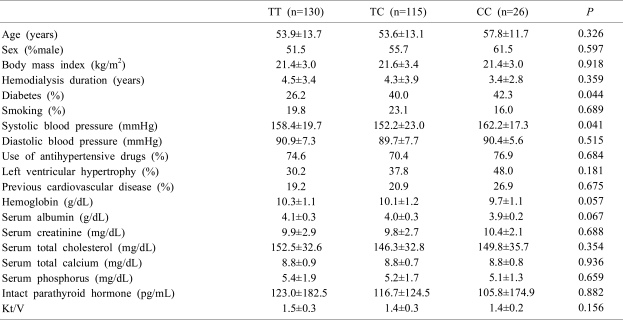
Table 3
Comparison of Clinical and Biochemical Characteristics of End-Stage Renal Disease Patients according to CYP11B2 Polymorphism
![]()
Go to :
Discussion
Our study was designed to test the hypothesis that the prevalence of renal failure may be influenced by gene polymorphism of the RAAS, especially aldosterone synthase gene polymorphism. In this cross-sectional study, we could not observe significant differences in the genotype and allele frequency of the CYP11B2 -344C/T polymorphism between controls and ESRD patients. Previous studies performed in Europe showed inconsistent results. Lovati et al. reported that there was no association between the CYP11B2 genotype and progression of renal failure among the ESRD patients15). On the other hand, Fabris et al. report ed that significant association was found between the CYP11B2 gene polymorphism and renal insufficiency in the hypertensive population16). They observed an increased proportion of CC genotype in hypertensive patients with renal damage compared with hypertensive patients without renal damage. The adjusted odds ratio was 3.89 for CYP11B2 -344C allele as a recessive effect. However, CYP11B2 genotypes were not in Hardy-Weinberg equilibrium among controls in Fabris and colleagues' report, so linkage disequlibrium in control subjects weakens a causal interpretation of these statistically significant findings. Controls in our study are of the normotensive healthy population and show similar allele frequency in comparison with another Korean study (T allele frequency 0.69)18). In the Korean population, there has been research aimed at evaluating the association between CYP11B2 polymorphism and hypertension18), myocardial infarction19), and risk of coronary in-stent restenosis20). To our knowledge, this is the first report about the CYP11B2 C-344T allele frequency in Korean ESRD patients.
Several studies of the association between this polymorphism and hypertension12, 21, 22), left ventricle size and mass13, 23), arterial stiffness24), and myocardial infarction14, 25) in the general population and hypertensive individuals with normal renal function have been performed. In ESRD patients, however, studies of association of CYP11B2 -344C/T polymorphism and left ventricular hypertrophy and cardiovascular morbidity are few. Our results did not show significant differences in left ventricular hypertrophy by EKG criteria and cardiovascular disease among the three genotypes in ESRD patients. We think this lack of association is due to not only limitation of the study, but also multifactorial etiology of cardiovascular morbidity in ESRD patients. The limitations of this present study are the insufficient statistical power as a result of a relatively small number of patients and the use of the EKG instead of echocardiographic examination for diagnosis of left ventricular hypertrophy. We obtained age and sex adjusted odds ratio using logistic regression methods because we could not match each individual case to his or her own control. It is also possible that the ESRD patients with high risk genotype may be excluded from the present study because of premature mortality due to cardiovascular influences by CYP11B2 polymorphism. Thus, further prospective investigation with sufficient statistical power is needed to explore the role of CYP11B2 polymorphism in the susceptibility of ESRD and cardiovascular effect in ESRD patients.
In conclusion, our findings do not support the hypothesis that CYP11B2 polymorphism is associated with prevalence of ESRD and suggest that CYP11B2 polymorphism may not be a genetic marker for cardiovascular morbidity in Korean ESRD patients.
Go to :
 XML Download
XML Download