

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
In ESRD patients, there have been significant increases in the prevalence of obesity among incident patients both in the USA and Europe12). In addition, AO appears to be problematic in peritoneal dialysis (PD) patients3). PD solutions contain high concentrations of glucose (>200 mmol/L)4). On average, 65% of intraperitoneally-administered glucose is absorbed during a 4 hour dwell, irrespective of the initial dialysate glucose concentration5). Therefore, PD patients appear to become more abdominally obese than HD patients6).
AO appears to be a risk factor for death in ESRD patients on hemodialysis (HD), as in the general population789). In PD patients, several studies have also reported AO to be a risk factor for mortality101112). Despite this, the follow-up periods of those studies were relatively short except for Lee et al.101112).
This study examined the effects of AO on the survival of PD patients. To accomplish this, the prevalence of AO in PD patients was assessed cross-sectional manner and followed up for 9 years at a single center.
Materials and Methods
This retrospective study was performed on ESRD patients on CAPD who had been followed up at the outpatient PD clinic, Inha University Hospital in Incheon, Korea. The inclusion criteria were 152 patients, who had received a cross-sectional nutritional assessment between September 2003 and March 2004. The CAPD system was a twin-bag. The CAPD prescription was 4×2 liter exchanges. In the case of a dialysis inadequacy, 5 exchanges were prescribed. The adequacy of CAPD was evaluated by measuring the weekly total Kt/V for urea and the creatinine clearance13).
The anthropometric measurements and nutritional assessments were performed by a well-trained dietitian at the PD clinic on the days they had visited for a monthly laboratory examination. Dialysate was drained from the abdomen. The height was then measured to the nearest 0.1 cm using a linear height scale. The body weight (BW) and fat mass were measured using the eight-point tactile electrode impedance method (Inbody 3.0; Biospace, Seoul, Korea). The body mass index (BMI) was calculated as the weight (in kilograms) divided by the square of the height (in meters). The waist circumference (WC) was measured at the umbilicus level at the end of expiration using a flexible plastic tape measure. The mean of two measures were used for analysis. AO was defined as a WC greater than 90 cm in males or greater than 80 cm in females14). The subjective global assessment (SGA) was used to evaluate the nutritional status15).
The patients were followed up until their death, kidney transplantation, transfer to HD or other hospital, or July 31, 2012. Their demographic, clinical and biochemical data was collected from the medical records. LDL-cholesterol was calculated by Friedewald equation16). Comorbidity was assessed using the age-adjusted Charlson comorbidity index (aCCI) score1718). Patients on CAPD of more than 2 years (n=46), lacking data of the WC(n=10) and had a follow-up duration of less than 6 months (n=10) after a nutritional assessment were excluded. Overall, 84 patients were included in the final analysis.
The primary outcome was the all-cause mortality. The secondary outcome was the cardiovascular-cause mortality from fatal cardiovascular events, which were defined as death from cardiovascular causes and stroke.
Statistical analysis was performed using SPSS for Windows Version 19.0 (SPSS Inc., Chicago, IL). The data is expressed as the mean±SD. The patients were classified as either with AO(AO group) or without AO(nAO group). The continuous variables between 2 groups were compared using an independent t-test. The nominal variables were assessed using a Chi-square test. The overall patient survival was estimated using the Kaplan-Meier method and a comparison of the outcomes were based on the log rank test. Kidney transplantation, technical failure and transfer to other hospitals were censored observations for patient survival analysis. Technical failure was defined as transfer to HD due to peritonitis, ultrafiltration failure, or mechanical problems. Mortality was analyzed using the multivariate Cox's proportional hazard model, in which all the significant variables from univariate analysis were included (in a backward manner). p<0.05 were considered significant.
Results
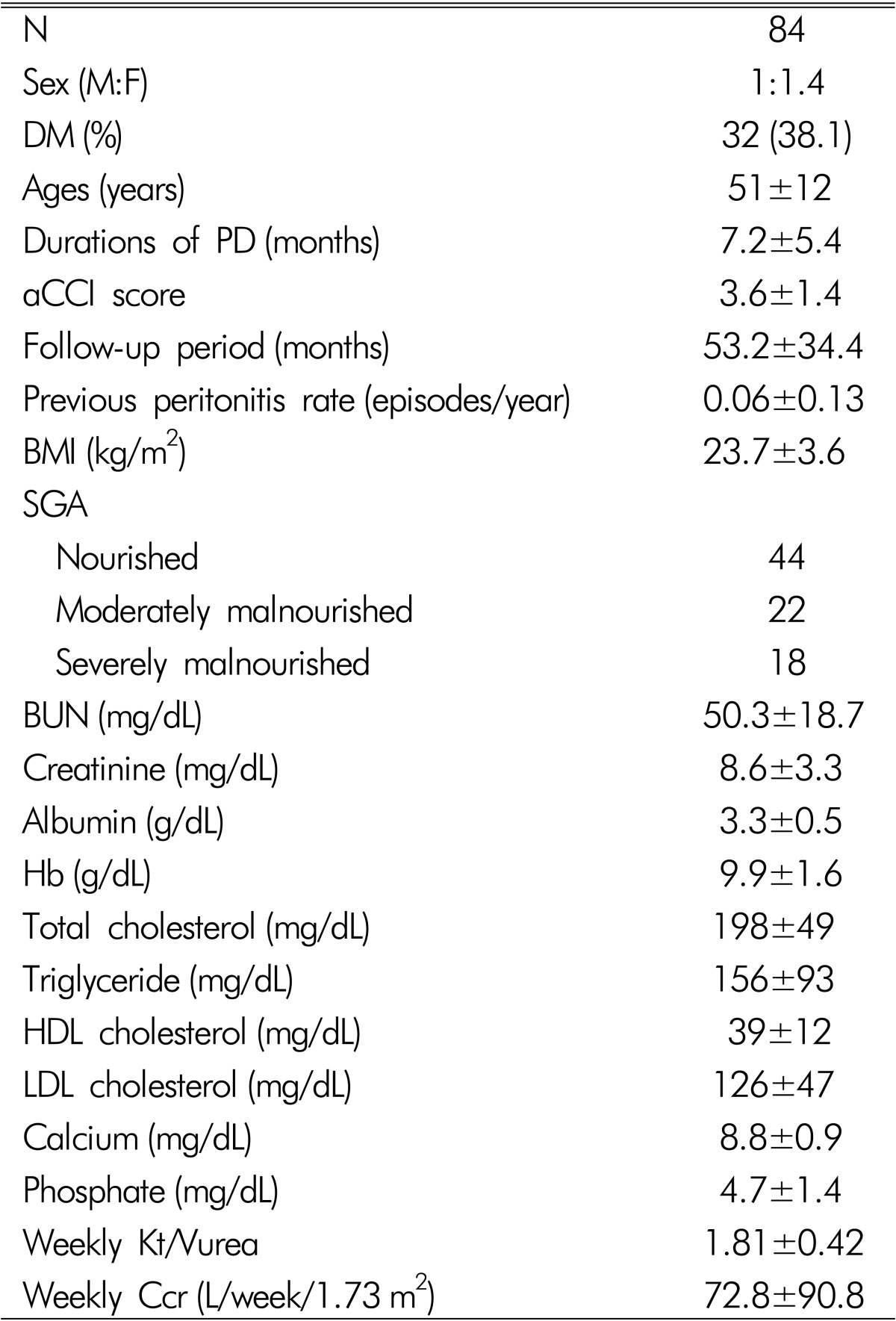
Table 1 lists the baseline characteristics of 84 subjects. The mean age of the subjects was 51±12 years. The male to female ratio was 1:1.4. Thirty two patients (38.1%) were diabetics. The previous durations of CAPD were 7.2±5.4 months. The aCCI score was 3.6±1.4. The BMI was 23.7±3.6 (range 17.2-33.6) kg/m2. The previous peritonitis rate was 0.06±0.13/year. According to the SGA, 44 were nourished, 22 were moderately malnourished and 18 were severely malnourished. The hemoglobin, BUN, serum creatinine, albumin, total cholesterol, triglyceride, LDL cholesterol, total calcium, and phosphate levels were 9.9±1.6 g/dL, 50.3±18.7, 8.6±3.3mg/dL, 3.3±0.5 g/dL, 198±49, 156±93, 39±12, 8.8±0.9, and 4.7±1.4mg/dL, respectively. The CAPD adequacies were examined in 53 patients. The weekly Kt/Vurea and creatinine clearance were 1.84±0.42 and 76.8±90.8 L/week/1.73m2, respectively.
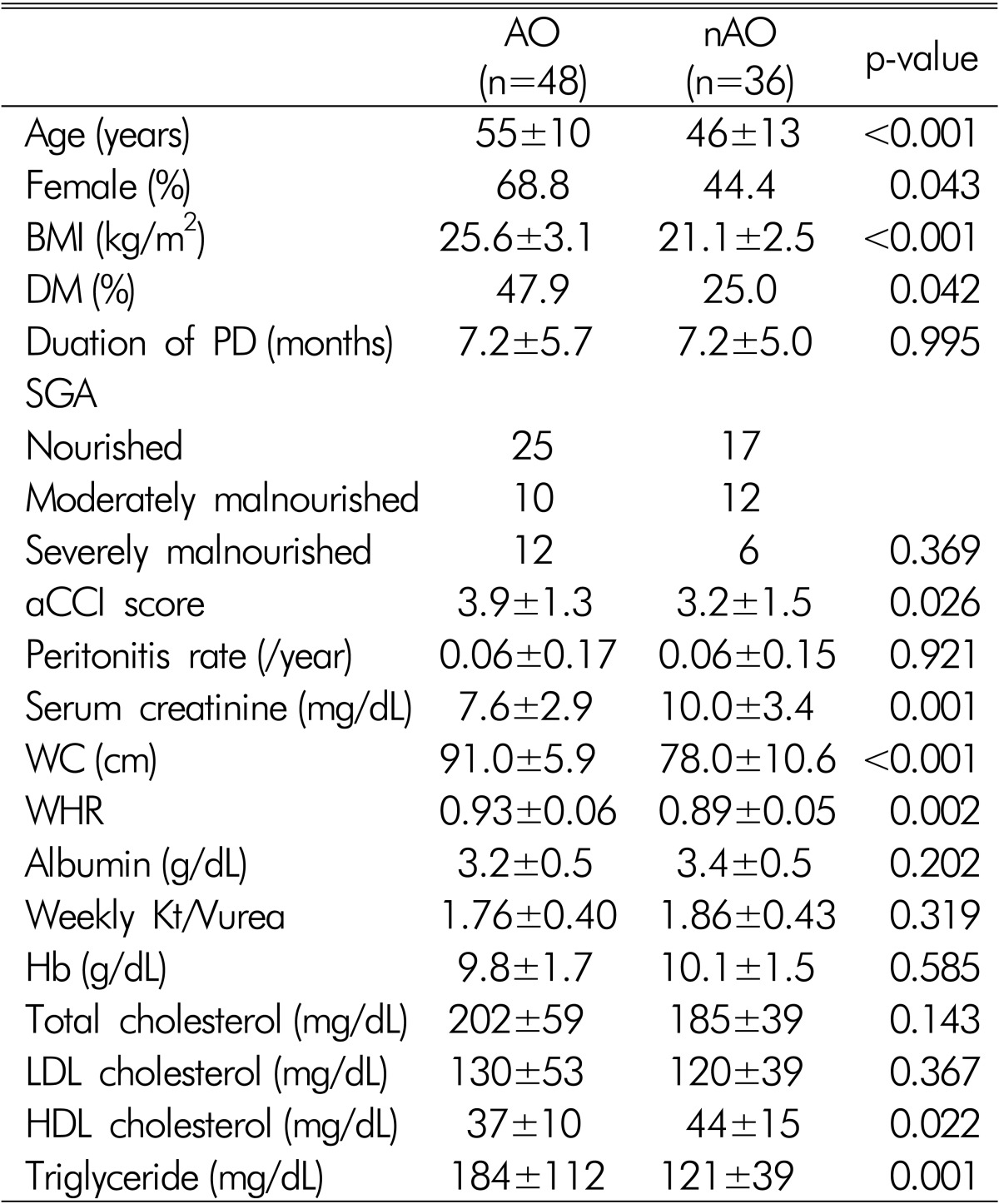
Among the 84 patients, the number of AO subjects was 48 (57.1%). The AO group was older, contained more diabetics, more females, and had higher aCCI scores, BMI and triglyceride, and lower serum creatinine concentration than the nAO group (Table 2). The previous duration of CAPD, nutritional status and peritonitis rates were similar in the AO and nAO groups.
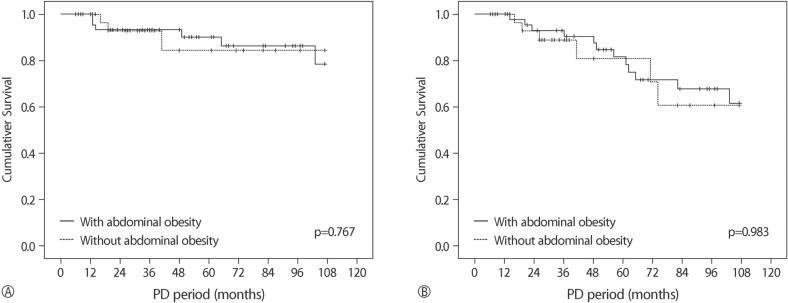
The follow-up duration was 53.2±34.4 months. At the end of the follow-up, eighteen (21.4%) were dead. Nine died of cardiovascular causes. The five year survival rate was 40.8%. Kaplan-Meier analysis showed that both all-cause (p=0.767) and cardiovascular-cause mortalities (p=0.983) were similar in the AO and nAO groups (Fig. 1).
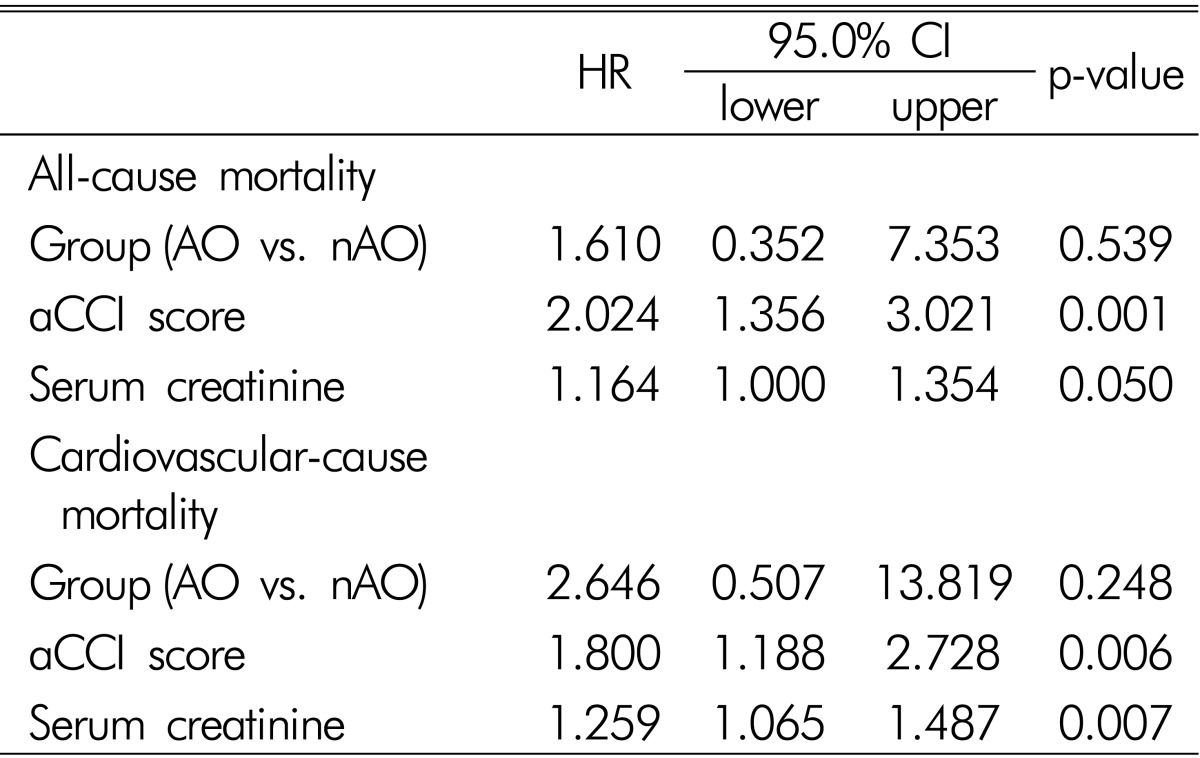
In multivariate analysis adjusted for sex, aCCI score, serum creatinine, triglyceride, HDL-cholesterol, group (AO vs. nAO), and BMI, aCCI score, and serum creatinine were found to be independent risk factors of all-cause and cardiovascular-cause mortality (Table 3).
Discussion
In this study, the presence of AO was not a risk factor for mortality in CAPD patients. The all-cause and cardiovascular-cause mortalities were similar in the patients with and without abdominal obesity. In the general population, obesity is a risk factor for CVD and is associated with increased mortality1920). On the other hand, there has been some controversy as to whether obesity is a risk factor for death in ESRD patients because several survival studies have suggested that a higher BMI is associated with improved survival2122). Currently, the fat distribution has different metabolic effects and abdominal fat is associated more closely with mortality than the total or peripheral fat23242526). Insulin resistance is induced by fat deposited intracellularly, and by proinflammatory cytokines, such as interleukins 1 and 6 and tumor necrosis factor α, secreted by adipose tissue2728). AO accentuates the problem, possibly because of the unusually high influx of portal fatty acids, cytokines and hormones into the liver from the omental adipocytes that are normally almost devoid of fat27). The effect of cytokines on the peripheral tissues with increased intracellular lipid also includes lower cellular insulin sensitivity27). The surge in lipids promotes the proliferation of the vasa vasorum of the arterial media, and apoptosis by the medial macrophages, with the further release of cytokines, resulting in hypertension, cardiovascular disease, diabetes mellitus, and others27).
AO appears to be a risk factor for death in ESRD on HD patients, as in the general population. Several studies have reported that AO is associated with mortality in ESRD on HD patients789). The PD patients may be at higher risk of developing AO compared to HD patients due to the use of glucose-based dialysis solutions10). The majority of patients experienced significant weight gain after the initiation of PD29). Visceral obesity was reported to be more common in PD patients than HD patients6). PD patients showed a 23% increase in the intra-abdominal fat area after initiating PD, despite the lack of a significant increase in weight or proportion of total fat mass30). WHR independently predicted mortality and CV events in 22 PD patients10). The WC and waist/hip ratio (WHR) were risk factors of all-cause and CV mortality in 537 ESRD patients9). Nevertheless, it was not known how many were undergoing peritoneal dialysis. Stolic et al. that the WC and BMI were predictors of death in PD patients11). In a prospective observational study, the sagittal abdominal diameter, which is a surrogate index of abdominal obesity, was also an independent predictor of mortality in 418 incident PD patients12).
In this study, the prevalent PD patients were followed up for more than 9 years after a cross-sectional assessment and the results were in contrast to other studies. Multivariate analysis revealed the presence of AO was not an independent risk factor for all-cause or cardiovascular-cause mortalities. Several possible causes of these differences can be speculated. The small number of subjects and short follow-up period used to evaluate the risk of death by AO are some reasons. Some studies, however, have reported lower number of subjects or shorter follow-up period than this study1011). Some studies support our results3132) Navaneethan et al. also reported that the presence of metabolic syndrome was not associated with mortality in patients with stages 3 and 4 chronic kidney disease (CKD)31). On the other hand, they used the BMI instead of the WC and the subjects were CKD patients not on dialysis. In 329 Chinese PD patients, the presence of metabolic syndrome was not a risk factor of death32). In a prospective study of 183 Chinese PD patients, abdominal fat was not associated with clinical outcomes such as CVD events or mortality33). In another prospective observational study with 117 Korean PD patients, increased abdominal fat at PD initiation was not a risk factor for poor outcome34).
The polymorphism in uncoupling protein 2 (UCP2) was reported to be associated with fat tissue accumulation during PD3536). There might be a racial difference in UCP2 gene polymorphism between Asians and Caucasians because no association between AO and mortality in PD patients were mostly reported from Asian subjects.
This study had several limitations. First, the AO was not measured using objective methods, such as computed tomography. Instead, the WC was used as an index of AO. Many indices, such as the WC, WHR, waist-height ratio, sagittal abdominal diameter, index of central obesity, and conicity index, were developed to express AO 263738394041). Among them, the WC is considered to be a simple anthropometric index of AO38). Furthermore, it was suggested that the WC alone could replace the WHR and BMI as a single risk factor for the all-cause mortality42). On the other hand, it showed low sensitivity when used as a single tool to identify older patients with either generalized or AO43). Furthermore, in PD patients, the WC may not reliably reflect the abdominal visceral fat content because the WC is affected by the presence of a catheter in situ, by lax skin conditions after repeated distention of the abdomen by PD fluid, and by potential residual PD fluid in the abdominal cavity44). The WC, however, was reported to be a reliable marker of AO in PD patients45), and was also associated with AO in CKD patients4546). Second, the subjects of this study were prevalent PD patients, not incident patients. Previous durations of CAPD were 21.5±22.3 (range 1-111) months. The absorption of 100-200 g of glucose per day from the conventional CAPD solution may promote obesity, glucose intolerance, insulin resistance, and the atherogenic lipid profile4). Therefore, patients with a longer duration of CAPD might have more AO. To reduce the effect of previous CAPD duration, in this study, the inclusion criteria was limited to dialysis vintage of less than 2 years and there were no differences in the previous duration of CAPD between the AO and nAO groups. Third, the effect of a bioincompatible solution was not considered. At the time of the cross-sectional nutritional assessment, the patients used a conventional CAPD solution because biocompatible solutions have been in use since the mid-2000s. Fourth, the peritoneal membrane transport characteristics were not included because at the initiation of this study, it was not regularly measured for all patients. Early studies found that the peritoneal membrane transport characteristics were important determinants of mortality in PD patients4748). Currently, it is controversial as to whether higher peritoneal transport characteristics at the start of peritoneal dialysis are associated with higher mortality4950). Fifth, the National Cholesterol Education Program(NECP) definition for AO is one of the most widely used definitions in the general population because of its simplicity and clinical relevance351). On the other hand, in this study, the definition of AO for the WC followed the International Diabetes Federation (IDF) criteria in 200514) because it considers ethnicity in its definition3). Sixth, there appeared to be selection bias of the subjects and the results of this study seemed to have low statistical power because it was a retrospective observational study at a single center. Despite this, the subjects were cared for by the same nephrologists for the follow-up period. Therefore, the results are less influenced by other factors, such as the center effect.
In conclusion, AO itself might not be a risk factor for mortality in PD patients. Nevertheless, further prospective studies with a larger number of patients will be needed to prove this.
 XML Download
XML Download