

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Hypokalemic paralysis is an important cause of acute flaccid paralysis that ranges from mild muscle weakness to severe paralysis with life-threatening cardiac arrhythmia and respiratory paralysis1,2). A number of underlying etiologies have been described, such as thyrotoxicosis, renal tubular acidosis (RTA), Gitelman-syndrome, barium poisoning, diuretics and diarrhea; however, in some cases, it is difficult to identify the exact etiology of hypokalemic paralysis. Misdiagnosis may lead to mismanagement, interference in appropriate treatments, and to failure for the prevention of recurrent attacks.
Hypokalemic periodic paralysis (HPP) is the most common cause of hypokalaemic paralysis in Caucasians3). HPP includes familial and sporadic form. Familial HPP is an autosomal dominant hereditary disorder while the cause of sporadic HPP remains unknown. Most cases of HPP in Western countries are the familial forms while most cases of HPP identified in Asians are sporadic4). Most Asian patients of sporadic HPP have been diagnosed as idiopathic HPP, also called primary HPP. In Asian population, however, the most common cause of hypokalemic paralysis is the thyrotoxic periodic paralysis (TPP)5).
We are aware that there are only a few reported documents regarding the etiology of hypokalemic paralysis in Korea. In this study, we report a spectrum of underlying etiologies, clinical features, and consequences for the patients of hypokalemic paralysis admitted at a single center in Korea. We also identify the differences in clinical parameters in relation to certain causes of the hypokalemic paralysis to guide a selection of appropriate treatment strategies and to take preventive measures against recurrent attacks.
Materials and Methods
1. Patients and methods
We retrospectively identified 34 patients with acute flaccid weakness due to hypokalaemia who were admitted to the Kyung-Hee Medical Center from Jan. 1, 2006 to the end of Dec. 2011. A definitive diagnosis of hypokalemic paralysis was confirmed based on the following criteria: (1) a transient and severe paralytic attack of the limb observed at the hospital by a physician, (2) hypokalemia during the paralytic attack(s) as defined by a serum potassium level: <3.5mmol/L. Patients with Guillaine Barré syndrome, acute transverse myelitis, cerebrovascular attack, chronic kidney disease or end stage renal disease on dialysis were excluded. Patients whose chief complaint was not the paralysis of the limb were also excluded.
A detailed medical history was obtained and neurological examination was performed on all patients. The family history of similar disease was recorded such as reports of weakness, thyroid disease, drug intake, diarrhea, vomiting, hypertension, and kidney disease. Muscle strength was assessed on a scale of 0 to 5 with using the Medical Research Council (MRC) scale. On admission, complete blood counts, blood urea nitrogen (BUN), serum creatinine, serum electrolytes (sodium, potassium, bicarbonate, chloride, calcium, inorganic phosphate), and thyroid function tests (TSH, Free T4 and T3 level) were obtained in all patients. If hyperthyroidism was suspected, auto-antibodies such as anti-thyroglobluin (anti-TG) antibody, anti-thyroid microsomal antibody (TMS-Ab) and thyrotropin binding inhibitory immunoglobulin (TBII) were measured. Patients of hyperchloremic metabolic acidosis with normal anion gap in the absence of gastrointestinal loss and a fasting urine pH >5.5 were regarded as having RTA.
The presence of metabolic alkalosis (serum bicarbonate >29mmol/L) with hypokalemia (serum potassium <3.0 mmol/L), hypomagnesemia (serum magnesium <2.5mg/dL), and hypocalciuria (urinary calcium <0.05mmol/kg/day) were regarded as indicative of Gitelman syndrome.
The patients were initially divided into 2 groups; the first were patients of idiopathic hypokalemic periodic paralysis and the second were those diagnosed as secondary hypokalemic paralysis, including TPP, diuretics or licorice induced hypokalemic paralysis, Gitelman syndrome, primary hyperaldosteronism, and distal RTA(dRTA). Because TPP has been recognized as the most common cause of hypokalemic paralysis in Asia and the clinical characteristics of TPP are more similar to idiopathic HPP than other causes of secondary hypokalemic paralysis, so we further divided the second group into TPP and non-TPP secondary HP.
2. Statistical analysis
Continuous variables were expressed as mean±standard deviation (SD) and were compared to using Student's T-test or Kruskal-Wallis test. Categorical variables were compared to using the Chi-squared test or two-by-K test. All statistical analyses were conducted by using the SPSS 17.0 statistical software (Chicago, IL, USA). Differences were considered significant if the p-value less than 0.05.
Results
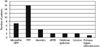
Those 34 patients with hypokalemic paralysis had a mean age of 38.59±16.92 years. Six were female. Seven of these patients (20.6%) were diagnosed as idiopathic hypokalemic periodic paralysis considered to be the sporadic form and 27 patients (79.4%) were categorized as having secondary hypokalemic paralysis. Of the secondary HP group, 16 patients (47.1%) were confirmed as having TPP. The secondary HP seen in the other patients was due to diuretics (n=4, 11.8%), licorice (n=2, 5.9%), Gitelman syndrome (n=2, 5.9%) or dRTA (n=2, 5.9%). Fig. 1 shows the spectrum of hypokalemic paralysis in our hospital. Table 1 shows the clinical characteristics of the affected patients in each of the three groups. The paralytic attack in all of those in the idiopathic HPP group was caused by the first event in their life time. In the TPP group, 11 patients (68.8%) had previously experienced mild weakness or paralysis of the limb, and 8 patients (50%) were showing repetitive paralysis before admission. In secondary hypokalemic paralysis without TPP, almost all of the patients (81.9%) had recurrences of the paralytic attack. In the idiopathic HPP and TPP groups, the mean recovery time (defined as resolution time of the paralysis or hypokalemia) was 9.29 hrs (SD±4.23) and 8.36 hrs (SD±1.24), respectively. On the other hand, in the secondary HPP group, the mean recovery time was 60.27 hrs (SD±31.13).
Table 2 presents the clinical features of patients in the thyrotoxic and idiopathic HPP group. The mean age was 31.38 years and 30.29 years, respectively. In TPP, 75% of the patients were in their 20-30'S (Fig. 2) and 50% of the patients had identifiable precipitating causes such as exercise, alcohol intake, carbohydrate-rich meal or upper respiratory infection (URI). Patients in the idiopathic HPP and TPP groups had similar clinical features.
Almost all patients (87.5%) with TPP recovered within 24 hours, but only 57.1% of the patients with idiopathic HPP recovered within this time period. Among the patients of the idiopathic HPP group, the paralytic attack usually happened in the morning or afternoon, but among the TPP group, the paralytic attack mainly occurred in the afternoon or while in sleep.
Table 3 shows the clinical features of TPP in this study. From among 50%(8/16) of the patients, clinical signs and symptoms of hyperthyroidism were absent at the time of the TPP diagnosis. The mean serum TSH level was 0.11±0.56 µU/mL (reference range: 0.30-4.00 µU/mL) in 16 patients. The serum T3 and FT4 levels were 247.75±83.38 ng/dL (reference range: 80-200 ng/dL) and 3.12±1.23 ng/dL (reference range: 0.77-1.94 ng/dL), respectively. Among the TPP group, only 3 out of the 16 patients (18.6%) had a previous history of hyperthyroidism. Two patients were poorly compliant with their medications and 1 patient was in a euthyroid state despite having a TSH level lower than the reference range. Of the 16 patients with TPP, 13 (81.3%) had clinically overt hyperthyroidism and Graves' disease at presentation while the other 3 (29.7%) had sub-clinical hyperthyroidism. Either positive TBII or anti-TG antibodies, or both were detected in all patients diagnosed with Graves' disease. After discharge, 2 out of 3 patients with sub-clinical hyperthyroidism were diagnosed as subacute thyroiditis.
Discussion
The episodes of hypokalemic paralysis of 27 (79.4%) from among the patients in our study were secondary to the pre-existing condition, including dRTA, Gitelman syndrome, primary hyperaldosteronism, diuretic or licorice induced HPP, and thyrotoxicosis. Idiopathic (primary) hypokalemic periodic paralysis was occurred from only 20.6% of the patients. Secondary hypokalemic paralysis was due to thyrotoxicosis from 47.1% of the patients; diuretics from 11.8%, and dRTA, Gitelman syndrome and licorice each represented 5.9%, and primary hyperaldosteronism from 2.9%. The etiology of hypokalemic paralysis has been shown varied across from different ethnic and geographical areas6-7). In a study from Taiwan, the majority of hypokalemic paralysis cases were secondary to pre-existing conditions (68%), although some sporadic and familial cases were identified. The underlying etiologies in that study included TPP (40.2%), sporadic (29.8%), familial (2.1%), primary aldosteronism(6.2%), renal tubular alkalosis, Bartter and Gitelman syndrome (6.2%), diuretic use (3.1%), and ingestion of toluene blue (3.1%)4), which is consistent with previous studies demonstrating TPP as the most common cause in Chinese and Japanese patients. Contrastingly, in Caucasian and Indian, familial HPP is the most common cause of hypokalemic paralysis, whereas in the Asian population, TPP is the most common cause5-6,14). There had been a paucity of reports documented on the etiology of hypokalemic paralysis in Korea, and therefore this might be the first to report that TPP is the most common cause of hypokalemic paralysis in Korea.
Earlier work has shown that mutations in the CACNA1S gene, which encodes the alpha 1 sub-unit of the skeletal muscle L-type voltage-dependent calcium channel, are responsible for the majority (70%) of the cases of familial HPP8,9). Missense mutations in the SCN4A gene, which encodes the skeletal muscle voltage-gated sodium channel alpha sub-unit, account for approximately 10% of the cases. Each mutation has different penetrance of phenotype, which also depends on gender10-11). Several Korean cases of familial HPP have been reported, but cases of previously identified gene mutations are rare. Even without genetic analysis associated with calcium channel or sodium channel in this study, the idiopathic HPP in our study could be regarded as a sporadic form in view of the absence of the familial history or previous symptoms. This is consistent with previous reports that most of the HPP patients in Western countries were of familial forms, whereas those reported from Asia were predominantly sporadic4). This raises the possibility that HPP in different ethnic settings may be linked to different types of mutations or to different environmental factors12). We were not able to investigate for the presence of mutation in patients with idiopathic HPP, and it seems clear that more genetic studies should be necessary.
We divided the patients with secondary hypokalemic paralysis into two groups, because TPP was clearly the most common cause of hypokalemic paralysis in Korea and it had a distinct clinical character from the other causes of secondary HP. The recurrence of paralytic attacks, presence of respiratory paralysis as a clinical feature, and most serum electrolyte (sodium, creatinine, inorganic phosphate or magnesium) levels were similar in all groups. There were significant differences in the serum potassium and serum calcium levels, and in the required potassium for the improvement among the three groups. In accordance with earlier reports, patients of secondary hypokalemic paralysis required a larger amount of potassium for the clinical improvement and had a longer recovery time compared with those who have idiopathic HPP or TPP13). Patients of secondary hypokalemic paralysis had a significantly negative total body potassium balance, whereas idiopathic HPP and TPP were associated with only intracellular shift of potassium, thus requiring a less amount of supplemental potassium14).
The precipitating causes of paralytic attacks were similar across all groups, including exercise, URI and alcohol intake. The patient's ages at first attack were also similar. Premoni- tory symptoms such as mild weakness and paralysis of both lower limbs, were more common in the TPP group than the idiopathic HPP group, which may represent one of the most important clinical differences between two groups.
The incidence of TPP among Asians, the most frequently affected population, is approximately 2%. While previously TPP was largely unknown in the West, the number of reported cases in Western countries has increased recently15). All reported TPP patients were sporadic cases without a family history of TPP, with the exception of one patient. This feature is important for differentiating TPP from familial hypokalemic periodic paralysis, which is more common among Caucasians16). Since most cases of idiopathic HPP in Korea were the sporadic forms, it seemed difficult to distinguish between TTP and the idiopathic HPP only by means of the presence or absence of familial history and the previous symptoms.
Despite the higher female incidence of thyrotoxicosis, TPP predominantly appears to affect males, and the ratio of male to female is 20:1.16 All of our cases were male. The youngest case was 16 and the oldest was 52 years old; most of the cases appeared between in the third or forth decades of life. No relationship between the age-onset of the disease and the complete recovery time was found in our study. The reasons for the male preponderance and the tendency of TPP onset between 20-40 years old remains unclear17-18). In hyperthyroid males, significantly increased plasma testosterone levels have been reported19). In Graves'disease, the plasma concentration of 17-β-estradiol is increased in males but remains unchanged in females20). The potassium channels in smooth muscle cells are activated by testosterone and estrogen in animal studies21,22). Furthermore, the age distribution of TPP patients coincides with the commonly observed age distribution of not only hyperthyroidism but the rapid increase in testosterone production. However, currently, we do not have any concrete evidence to prove the effects of sex hormones and potassium channels on TPP; this might be an important direction for future research.
We should take note of that Graves' disease was also the most common cause of TPP in our study. Subacute-thyroiditis was also an etiological factor in our study. A thyrotoxic state is generally considered necessary for the induction of TPP, however, some studies have reported that acute paralysis had occurred in even in a euthyroid state after a treatment of the thyrotoxicosis25-26). Most of the patients included in our study had overt thyrotoxicosis while 3 patients had only subclinical thyrotoxicosis. We suggest that doctors should consider TPP even if a patient is under taking medicine for thyrotoxicosis or is having the possibility of subclinical hyperthyroidism, i.e., an apparent euthyroid state. Accordingly, those with hyperthyroidism and TPP should not be presumed to have Graves' disease, for some of them may experience hypothyroidism after subacute thyroiditis.
The patients with secondary HPP without TPP in our study required a longer recovery time compared with those who have idiopathic HPP or TPP. Those patients with secondary HP had a significant negative total body potassium balance, and required larger amounts of potassium compared with idiopathic HPP and TPP groups.
Because of the limitations on the retrospective data, the relatively small number of patients and restriction to a single center in this study, further prospective large-scale studies are required for delineating the spectrum of etiologies, clinical findings, treatment outcomes, and predictors of hypokalemic periodic paralysis.
In conclusion, our study revealed that, in Korea, idiopathic (primary) hypokalemic periodic paralysis occurred in 20.6% of the patients. The most common cause of hypokalemic paralysis in Korea was thyrotoxicosis (47.1%).




 XML Download
XML Download