

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Synovial sarcoma (SS) is a relatively common neoplasm accounting for 5% to 10% of all soft tissue sarcomas, typically occurring in younger patients between 15 and 35 years, predominately near the large joints of the extremities (60%–70% in the lower extremity).1) Contrary to its name, SS does not originate from the synovial cell, and although it arises from within the joint in less than 5% of all cases, it is considered to have the highest incidence among primary intra-articular malignancies.2) It typically presents as a slow-growing mass that may be indolent, and it is the most common sarcoma of the foot. Imaging may show a soft-tissue mass with sometimes presence of calcification, and on T2 magnetic resonance imaging (MRI) sequence there is typically a heterogeneous “triple-signal” (i.e., high, intermediate, and low intensity). Histologically, it presents most frequently as a biphasic form containing both a spindle cell and epithelioid components but it may also occur as monophasic, i.e., spindle cell pattern only. Management of SS consists of wide excision with adjuvant radiotherapy whereas chemotherapy may also improve survival. The 5-year survival rate is reported to range from 30% to 74%.3)
SS may often present with atypical clinical features of soft-tissue sarcomas causing a delay in diagnosis and management.4) Furthermore, misdiagnosis or unplanned tumor excision is also reported in patients with this type of malignancy. Management would be different if definitive diagnosis was established early enough and significant morbidity could be avoided.5) Most of the time, reoperation is inevitable in order to achieve wide excision with “free” margins due to the previously contaminated surgical “bed.”5)
The authors present a rare case of SS in a patient who had concurrent knee osteoarthritis and underwent total knee arthroplasty. An unplanned biopsy was sent and the diagnosis of intra-articular SS was established. The presence of SS was initially missed and the patient was subsequently treated with a wide resection, radiotherapy and revision knee arthroplasty with an endoprosthesis. To the authors' knowledge, this has not been reported in the English-language literature and it highlights that a high index of suspicion is mandatory in order to avoid a potentially disastrous clinical outcome. This is a case report and the IRB is non applicable. The patient provided written informed consent for print and electronic publication of this case report.
CASE REPORT
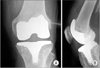
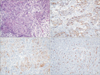
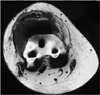
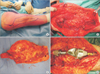
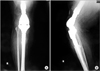
A 68-year-old female presented to an outside hospital complaining of long-standing right knee pain. There was no history of trauma and her past medical history was otherwise unremarkable. Four months prior, she had undergone bilateral knee intra-articular high molecular weight hyaluronic acid injections. Physical examination of her right knee revealed full but painful range of motion and tenderness especially on the medial compartment. Radiographs of the knee revealed radiographic characteristics of osteoarthritis including joint space narrowing and sclerosis (Fig. 1). The patient underwent total knee arthroplasty for management of knee osteoarthritis. Intraoperatively, there were extensive arthritic changes in all three compartments. At that time, the surgeons observed that the lateral part of the synovial membrane in close proximity to the quadriceps muscle was found to be thickened and had an associated “fatty mass.” A specimen was sent for pathology, but at the same time, the findings were attributed to reactive synovitis, secondary to knee arthritis and the ongoing total knee arthroplasty (posterior stabilized design) proceeded per routine (Fig. 2). One week postoperatively, pathology results showed a biphasic malignancy composed of a mixture of spindled mesenchymal cells with admixed glandular epithelial elements. Immunohistochemically, the tumor was positive for vimentin, CD99, keratins AE1/AE3, keratin 7, epithelial membrane antigen, focally positive for S100, keratin 19 and keratins 8 and 18 of the epithelial-like cells. The aforementioned morphologic and immunohistochemical findings were consistent with a biphasic SS (Fig. 3). The patient was subsequently referred to the Musculoskeletal Oncology Department at the University of Athens School of Medicine for consultation and further management. An MRI of the right knee showed a large soft-tissue mass on the anterolateral side of the distal thigh. The mass was extending into the substance of the vastus lateralis, presenting a heterogenous fusiform morphology. The mass was 7.2 × 8 × 6.2 cm, with irregular contrast enhancement. There was no evidence of regional cortical infiltration or any signs of an intramedullary inflammatory lesion (Fig. 4). Further evaluation of the patient with a computed tomography scan of the chest, abdomen and pelvis as well as a bone scan did not provide any evidence of metastatic disease. After appropriate preoperative planning, limb salvage surgery with endoprosthetic reconstruction was undertaken (Fig. 5). The patient was reoperated 28 days following the first operation. Given the fact that the knee joint was considered highly contaminated, a wide extra-articular tumor resection, including the site of the previous arthroplasty was mandatory. Accordingly, an extended medial fusiform incision including the previous incision and the patella was performed (Fig. 5A). En-bloc resection of the tumor included the entire knee joint (Fig. 5B and C). Nevertheless, the regional neurovascular structures were preserved and the residual bone defect was reconstructed using a modular knee megaprosthesis (METS modular implant system; Stanmore Implants, Borehamwood, UK) (Fig. 5D). Histology of the resected specimen confirmed the diagnosis of classic biphasic SS, whereas it demonstrated tumor-free wide surgical margins. In the early postoperative period, the extensive soft tissue resection resulted in wound closure complications and exposure of the endoprosthesis. The defect was treated successfully using a gastrocnemius rotational flap. The latter technique provided sufficient coverage to the knee endoprosthesis avoiding further complications or infection (Fig. 6). After wound healing, the patient was referred to the Medical Oncology Department to proceed with adjuvant therapy, but she declined any further treatment including chemotherapy or radiotherapy. She was therefore advised to stay under close medical surveillance. At the last follow-up, 8 years postoperatively, the patient demonstrated no signs of local recurrence or systemic disease. Additionally, there was no evidence of implant loosening (Fig. 7), while she ambulated satisfactorily with a walking stick.
DISCUSSION
SS is a microscopically distinctive subtype of soft-tissue sarcoma that occurs predominantly near the large joints of the extremities with a predilection for young adults.1) The term “synovial” is a widely recognized misnomer, as this tumor has no clear synovial differentiation. Although arising from the joints in less than 5% of cases, it presents as the most common primary intra-articular malignancy.6) Clinical features are not characteristic, and for this reason delay in diagnosis and management may be significant.4) Misdiagnosis has been reported in patients suffering from this malignancy.5) In such cases, reoperation is often unavoidable in order to achieve wide tumor-free margins in the setting of a previously contaminated surgical “bed.”5)
There have been reports of misdiagnosed SS in the knee,267) but none in the context of total knee arthroplasty. We present a case of SS that was missed at the time of a primary total knee arthroplasty. There was no index of suspicion for malignancy as the clinical and radiographic evidence was typical of primary osteoarthritis in the knee. Intraoperatively, the presence of a “fatty mass” was noted close to the quadriceps but this was attributed most likely to reactive synovitis. However, the surgeons did send a biopsy of the mass, which turned out to be SS.
Friedman et al.2) recently reported the case of a 26-year-old patient with an intra-articular SS located in the posterolateral compartment of the right knee in order to highlight the rarity of the intra-articular component of the disease as well as its nonspecific features. Jamshidi et al.6) reported a similar case that was initially diagnosed as a meniscal cyst and treated arthroscopically. Similar to our case, the patient had no findings on the radiographs. MRI presented the misleading features of a well-defined cyst in the anterior horn of the medial meniscus; these findings did not raise concerns during initial assessment. After arthroscopy, the patient underwent reoperation with wide excision of the tumor bed.6) In the same setting, a study that examined the characteristics of misdiagnosed SS reported that these tumors are quite often mistaken for neurogenic tumors in the upper limb and for cysts in the lower limb.8) McLain et al.7) reported the case of a patient with SS of the left knee that was initially misdiagnosed as pigmented villonodular synovitis, even after synovectomy and histological evaluation of the collected synovial fragments. All this evidence combined with our case reinforce the concept that SS may be misdiagnosed or diagnosed late, because they do not present the typical features of soft-tissue sarcomas.4) Management in such cases consists of reoperation to provide wide re-excision of the “contaminated” surgical wound, eventually followed by adjuvant radiotherapy and/or chemotherapy depending on the margins achieved, the stage of disease and the time of reoperation. In a study comparing planned and unplanned soft tissue sarcoma resections, Qureshi et al.9) observed an increased rate of local recurrence in patients with unplanned resections that was secondary to the extensive “contamination” of the surgical boundaries. On the other hand, Fiore et al.10) in their study have reported similar outcomes between primary tumor resections and reresections, probably due to their copious reoperation strategies to provide very wide margins and include any possible residual malignant tissue. Our patient did not receive any unplanned tumor excision in the first operation but the surgical site of total knee arthroplasty was definitely highly “contaminated.” The prompt reassessment and the wide margins achieved by the extra-articular knee resection probably played a decisive role in the final favorable outcome.
The case described in this report is quite rare and highlights the importance to include a potential malignancy in the differential diagnosis of knee pain. While there are no guidelines to indicate routine advanced imaging in unambiguous cases, plain radiographs must be assessed with a high index of suspicion. Intraoperatively, sound clinical judgement should include a low threshold for obtaining a biopsy in doubtful cases in order to minimize delay in definite diagnosis and treatment.


 XML Download
XML Download