

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Little leaguer's shoulder, which was first described by Dotter1) in 1953, is a syndrome in which the proximal humeral epiphyseal plate of an adolescent athlete is injured by excessive rotational stress on the proximal physis during throwing motion.2) Conservative treatment usually resolves the symptoms.2) However, radiographic follow-up studies of this syndrome have not been available, even though fractures of the epiphyseal plate during childhood may cause premature closure that results in limb deformity.
Humeral retroversion in throwing athletes has been reported to be greater on the dominant side than on the nondominant side.345) The increased humeral retroversion is thought to result from repetitive throwing motion. However, the degree of increased humeral retroversion is various (ranging from 8.3° to 17°),345) suggesting that other factors may affect humeral retroversion in throwing athletes. Here, we hypothesized that little leaguer's shoulder, which is a stress fracture or Salter-Harris type I injury of the proximal humeral physis,6) may cause three-dimensional (3D) deformity of the proximal humerus. The purpose of our study was to document the healing process of little leaguer's shoulder using 3D computed tomography (CT).
CASE REPORT
Humeral deformity in a 15-year-old male baseball player who had been diagnosed with little leaguer's shoulder at aged 13 was evaluated by 3D CT. The study was approved by the Institutional Review Board of Osaka Medical College (IRB No. 2251) and performed in accordance with the principles of the Declaration of Helsinki. Informed consent that his data would be submitted for publication was obtained from the patient. He had begun playing baseball at 9 years old and had always been an outfielder. When the patient was 13 years old, he had developed shoulder pain during throwing motion as a result of little leaguer's shoulder. Our criteria of little leaguer's shoulder are physeal widening in the proximal humerus on the dominant side on plain radiographs (Fig. 1) and tenderness at the proximal physis. At that time, 2 months of rest from playing baseball had resolved his symptoms, and he had successfully returned to his previous level of activity (Fig. 1).
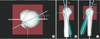
With the patient's and his parents' approval, both of his proximal humeri were scanned by CT with the subject in the supine position (16 detector rows, 1.00-mm-thick slices, 120 kV, 200 mA; Hitachi, Tokyo, Japan). Data were saved in DICOM (Digital Imaging and Communications in Medicine) format and sent to a workstation (Precision 6700; Dell, Round Rock, TX, USA). Three-dimensional surface models of both proximal humeri were reconstructed by using Synapse Vincent (Fuji Film, Tokyo, Japan) and custom software (OV; Department of Orthopedic Biomaterial Science, Osaka University, Osaka, Japan) (Fig. 2).37)
We analyzed the valgus–varus, flexion–extension, and rotational deformation of the dominant humerus by comparing a model of the dominant side with a superimposed mirror-image model of the nondominant side. All superimpositions were performed semi-automatically by using the iterative closest-point algorithm for surfacebased registration.37) First, the humeral head proximal to the epiphyseal plate was superimposed on the corresponding mirror image of the nondominant side. Then the valgus– varus and flexion–extension deformation was evaluated by comparing the longitudinal axis of the humeral shaft between the dominant and nondominant sides. Rotational deformity was measured by comparing the humeral head axis, which is perpendicular to the articular margin of the humeral head, between the dominant and nondominant sides.
Although the radius of the humeral head was almost the same on both sides (dominant side, 24.4 mm; nondominant side, 24.5 mm), the shapes of the greater and lesser tuberosities differed between the dominant and nondominant humeri (Fig. 3), as did the proximal humerus just inferior to the physis. Humeral retroversion was increased by 27.1° on the dominant side compared with the nondominant side (Fig. 4A). Compared with the nondominant shaft, the dominant humeral shaft was deformed in the varus direction (9.4°), leading to a decreased neck–shaft angle (dominant side, 127.5°; nondominant side, 135.1°), and it was also deformed in the extension direction (21.0°) (Fig. 4B and C).
DISCUSSION
Little leaguer's shoulder is considered to be a stress fracture or Salter-Harris type I injury of the proximal humeral physis.6) Although a traumatic fracture of the proximal humeral epiphysis typically leads to shortening of the humerus and malunion with residual angulation even after healing,89) humeral deformity in baseball players with little leaguer's shoulder has not been reported previously. The scarcity of follow-up studies may reflect both the infrequency of residual functional problems after conservative treatment of little leaguer's shoulder and technical difficulty of accurately measuring humeral deformity with plain radiography. Here, we used 3D CT to analyze humeral deformity after successful conservative treatment of little leaguer's shoulder.
Humeral retroversion in throwing athletes has been reported to be greater by 8.3° to 17° on the dominant side than on the nondominant side.345) However, retroversion in our patient (27.1°) was markedly greater than that in previous reports. Furthermore, varus and extension deformation of the humerus has not been previously reported as a throwing-related outcome. Therefore, the combination of increased retroversion and varus and extension deformities in our patient might have resulted from stress fracture or Salter-Harris type I injury of the proximal humeral physis (little leaguer's shoulder) rather than from repetitive throwing.
Increased humeral retroversion in overhead throwing athletes is thought to be an adaptive change to the throwing motion.4) However, little leaguer's shoulder, a common throwing injury in adolescent athletes, apparently increases humeral retroversion rapidly, that is, within just a few years of starting the sport. Furthermore, the humeral deformity in our patient included not only increased humeral retroversion but also varus and extension deformities. These changes suggest that, even after successful treatment of little leaguer's shoulder, the humeral axis deviates beyond the rotational axis of the humeral head, theoretically leading to inefficient movement and increased torque of the humerus during throwing motion. Anz et al.10) reported that higher levels of torque at the shoulder and elbow resulted in an increased risk of injury. Therefore, humeral deformity in overhead throwing athletes may not always be due to adaptive mechanisms. To clarify how little leaguer's shoulder causes humeral deformity, a cohort study is necessary.
Our perhaps unusual application of 3D CT in this case was made in response to a request from the patient and his parents. In addition, the patient already retired from baseball, so the long-term effects of humeral deformity after little leaguer's shoulder in this patient remain unclear. Further studies that assess the relationship between humeral deformity in little leaguer's shoulder and throwing injury are required.
Other potential causes of humeral deformity need to be considered, such as congenital deformity or deformity following other injuries. In our case, the patient had neither any disease that may cause congenital deformity nor any past history of trauma or surgery in the shoulder joint. Therefore, we believe that the humeral deformity in this case resulted from little leaguer's shoulder.
In conclusion, this case demonstrates that little leaguer's shoulder can cause markedly greater humeral retroversion than has been reported previously and also result in varus and extension deformation of the humerus. These findings suggest that humeral deformity in overhead throwing athletes does not always solely reflect adaptation to throwing. More studies are needed to assess the relationship between humeral deformity after little leaguer's shoulder and subsequent throwing injuries.



 XML Download
XML Download