

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Anterior cruciate ligament reconstruction (ACLR) is a common orthopedic procedure. The EndoButton Continuous Loop (Smith & Nephew, Andover, MA, USA) is a popular device used for femoral fixation of soft tissue anterior cruciate ligament grafts. Introduced in the early 1990s, the EndoButton allows for a femoral cortical suspensory fixation and has been shown to be biomechanically stronger than interference screws.1) Associated complications from EndoButton usage are rare. Some complications include the incomplete passage of the EndoButton and soft tissue interposition between the EndoButton and the femoral cortex resulting in loss of tension after surgery. Intra-articular displacement of the EndoButton after single bundle ACLR is an even rarer complication and has been reported only twice in the literature.23)
We present a case of intra-articular displacement of EndoButton following anterior cruciate ligament reconstruction and highlight an intraoperative measure that may prevent such a complication.
CASE REPORT
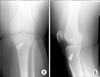
A 24-year-old man presented to our institution with left knee pain and instability after standing up from a seated position. The patient had suffered a ruptured left anterior cruciate ligament 36 months ago and had undergone an anterior cruciate ligament reconstruction at another institution. A single bundle ACLR using a 9-mm and 4-stranded hamstring autograft was performed. Immediate postoperative X-rays revealed an anterior placement of the femoral tunnel (Fig. 1). After the initial surgery, the patient did not have any symptoms of pain or instability. Three years later, the patient attempted to stand up from a seated position and felt a sudden pain in his left knee. This was associated with an immediate knee effusion. Subsequently, he complained of instability and pain in his left knee. On clinical examination, the patient had a positive Lachman and anterior drawer tests. Radiographic imaging revealed an intra-articular displacement of the EndoButton into the posterolateral recess of the knee joint (Fig. 2). Magnetic resonance imaging (MRI) revealed a failure of the ACL graft (Fig. 3). A revision anterior cruciate ligament reconstruction was performed for the patient.
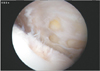
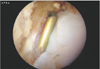
Intraoperatively, it was noted that the femoral tunnel exit was located on the anterior aspect of the lateral femoral condyle, within the suprapatellar pouch. The suture loop had failed and resulted in intra-articular displacement of the EndoButton (Fig. 4). An intraoperative image intensifier was utilized to locate the EndoButton which had been wedged between the posterior aspect of the lateral tibial plateau and the capsule (Fig. 5). The EndoButton was removed via posterior portals. A revision anterior cruciate ligament reconstruction with allograft using a transportal technique was then performed.
DISCUSSION
The EndoButton is commonly used for femoral fixation of the graft and intra-articular displacement following failure is rare. Poor placement of the EndoButton during initial fixation may predispose to such a complication. An anteriorly placed femoral tunnel results in EndoButton placement within the suprapatellar pouch. Improper placement of the femoral tunnel is believed to be a common cause of failure of ACLR for several reasons.4) Firstly, the femoral tunnel that is placed too anteriorly results in a vertically oriented graft and increased stressed on the graft during flexion. Secondly, placement of the femoral tunnel within the suprapatellar pouch results in persistent synovial fluid infiltration through the cortical hole. Synovial fluid can result in an increased level of inflammatory cytokines that stimulate osteoclastic activity within the bone tunnel.5) This leads to tissue damage, delay of graft incorporation, and subsequent tunnel widening. Finally, placement of the EndoButton too close to the patellofemoral joint may predispose it to shearing forces during normal knee kinematics. Then, impingement of the EndoButton can occur and this, resulting in weakening of the suture loop with eventual failure.
The mode of failure of the EndoButton in our case is via the suture component. This is similar to the previous two published case reports. In the previous two case reports, the EndoButton tapes were tied intraoperatively and failure occurred via suture loosening. In our case, a continuous loop was utilized and the failure was secondary to a ruptured suture loop. It seems that poor graft incorporation resulted in increased stress on the EndoButton fixation. This led to eventual failure of the suture loop 36 months after surgery.
Removal of a displaced intra-articular EndoButton can be challenging. The EndoButton is relatively small and may migrate freely with knee motion. Intraoperative fluoroscopy should be utilized if the surgeon is unable to locate the EndoButton. The use of posterior portals and a 70° arthroscope may be helpful if the EndoButton is found to be within the popliteal space.
We believe that anterior placement of the EndoButton at initial surgery may be a predisposing factor for intra-articular displacement of the EndoButton. It is recommended to check the EndoButton position intraoperatively to avoid such a complication, especially for the unexperienced surgeon.


 XML Download
XML Download