

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Chronic radial head dislocation in children, of both traumatic and congenital types, is a challenge for the physician. Treatment options range from nonsurgical treatment, ulnar osteotomy,1234567) ulnar and radial osteotomy,89) annular ligament reconstruction1011121314) to ulnar osteotomy and annular ligament reconstruction.9151617) However, the literature does not provide an optimal procedure for cases which have gone untreated for several years with various deformities. When the normal anatomy of the proximal radius and ulna is changed, stable reduction of the radial head cannot be obtained by a single osteotomy performed to correct anterior bowing of the ulna (caused by a previous Monteggia fracture). In the forearm where both the radius and ulna rotate on one axis, an uncorrected deformity in one bone may influence the other. Therefore, forearm rotation will deteriorate after surgery if all deformities in both bones are not corrected.
Although surgical treatment for traumatic dislocation primarily depends on radiographic findings, there have been no detailed studies on radiographic changes of the radius and ulna. In 22 patients whose traumatically dislocated radial heads were surgically reduced by traditional methods, we analyzed pre- and postoperative anteroposterior (AP) and lateral radiographs to shed light on the clinical efficacy of surgical treatment.
METHODS
We retrospectively reviewed radiographs of patients with traumatic radial head dislocation. Informed consent for participation in the study was obtained from all patients or parents. We evaluated 22 forearms (22 patients, nine females and 13 males) with traumatic anterior dislocation of the radial head. The mean age of patients at the time of dislocation was 8.3 years (range, 3 to 15 years); the mean duration of dislocation was 14.9 months (range, 1 to 96 months); and the mean age at the time of surgery was 9.6 years (range, 5.7 to 18 years). Each subject had two radiographs of the affected side before and after operation (a mean of 7.7 years [range, 3 to 13 years] after surgery). An AP radiograph taken with the elbow in full extension and the forearm in supination and a lateral radiograph taken with the elbow in 90° flexion and the forearm in neutral rotation were selected from the picture archiving and communication system.
Measurement of Radiographic Parameters
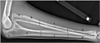
On AP and lateral radiographs, we divided the forearm into three equal parts (the proximal, middle, and distal thirds) and analyzed parameters we devised (described below) to evaluate deformities in each part (Figs. 1 and 2). Two of the parameters, maximal radial bow (MRB) and location of MRB (LMRB), were only measured from the AP view (Fig. 3) because of overlapping of the radius and the ulna in the lateral view. Parameters were measured using tools in the Marosis m-view 5.4 software (Marotech, Seoul, Korea).
Proximal third
Proximal radial tilt angle (PRTA) represents the angle between the rotational axis of the forearm (AA’, from the center of the radial head to the center of the distal ulna) and the axis of the radial neck (a). The axis of the radial neck is from the center of the radial head to the center of the radial neck which is just on the apex of the bicipital tuberosity.
Proximal ulnar tilt angle (PUTA) is the angle between the rotational axis of the forearm (AA’) and the axis of the proximal ulna (e). The axis of the proximal ulna is from the center of the ulna which is just below the coronoid process to the proximal third of the ulnar shaft.
Proximal radioulnar angle (PRUA) is the angle between the axis of the radial neck (a) and the axis of the proximal ulna (e).
Middle third
Middle radial tilt angle (MRTA) represents the angle between the rotational axis of the forearm (AA’) and the axis of the middle radius (c). The axis of the middle radial shaft is from the center of the junction of the proximal and middle radius to the center of the junction of the middle and distal radius.
Middle ulnar tilt angle (MUTA) represents the angle between the rotational axis of the forearm (AA’) and the axis of the middle ulna (f). The axis of the middle ulnar shaft is from the center of the proximal-middle ulna junction to the center of the middle-distal ulnar shaft junction.
MRB is the maximal distance (C to C’) from the ulnar side of the radius to the line connecting the bicipital tuberosity and the most ulnar aspect of the radius at the wrist (BB’).
LMRB is a ratio of the distance from the bicipital tuberosity to the point of MRB (B to MRB) to the distance from the bicipital tuberosity to the most ulnar aspect of the radius at the wrist (B to B’).
Distal third
Distal radial tilt angle (DRTA) represents the angle between the rotational axis of the forearm (AA’) and the axis of the distal radius (d). The axis of the distal radius is from the center of the junction of the middle and distal radius to the center of the distal radius.
Distal ulnar tilt angle (DUTA) represents the angle between the rotational axis of the forearm (AA’) and the axis of the distal ulna (g). The axis of the distal ulna is from the center of the junction of the middle and distal ulna to the center of the distal ulna.
Analysis of Deformities
We compared the nine parameters listed above between the affected and the unaffected sides, both before and after surgical treatment. The patients were divided into two groups according to the duration of dislocation. A cutoff value (4 months) was selected so that the number of patients in the two groups was similar. There were 10 patients with a duration of 4 months or less in one group and 12 patients with a duration of more than 4 months in the other group. We assessed differences between the groups.
Range of Motion of the Elbow and Forearm
Preoperative range of motion (ROM) of the elbow and forearm was obtained from the medical records, while postoperative ROM was measured at the last follow-up. ROM included flexion-extension, pronation, and supination measured with a hand-held goniometer using standard methods.
Surgical Treatment
Surgical treatment included various procedures.18) Open reduction of the radial head, debridement of soft tissues between the radial head and capitellum, radial shortening when the radius was elongated, and annular ligament reconstruction using a pedicled central tendinous strip of the triceps were the main procedures on the radial side. Rotation of the proximal part of the osteotomized radius19) and/or radial head arthroplasty were often performed when congruency between the radial head and the capitellum and/or stability of reduction were judged insufficient. Ulnar flexion osteotomy to correct anterior ulnar bowing was performed at the proximal site or at the location of maximal deformity in the diaphysis. Notchplasty in the proximal ulnar notch for the radial head (excision of osteophytes or hypertrophied bone) was performed when it improved stability of reduction of the radial head and/or forearm movement. Osteotomy sites in the radius and ulna (proximal or middle) were decided before the operation based on comparison of the AP and lateral radiographs of the unaffected and affected sides. Osteotomy sites chosen to correct deformity in the ulna were proximal in 12, middle in six, and distal in one. Combined radial osteotomy and/or shortening were performed in 10 cases (nine middle and one proximal). The amount of radial shortening was decided preoperatively by measuring the distance from the coronoid process to the displaced radial head in the radiograph, or during surgery by measuring the overlapping length of the osteotomized radius after radial head reduction. Selection of all procedures for each patient was decided by the senior author (HTK).
Statistical Analysis
Paired t-tests were used to compare parameters between the affected and the unaffected sides. The Mann-Whitney U-test was used to compare parameters between two groups of patients separated by the duration of dislocation. To compare values of ROM before and after surgery, we used a Wilcoxon signed-rank test. All variables are reported as means and standard deviations. Values of p < 0.05 were considered statistically significant. All data analyses were performed using IBM SPSS ver. 24.0 (IBM Corp., Armonk, NY, USA).
RESULTS
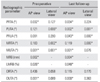
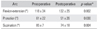
The values of all parameters measured on the unaffected side and on the affected side, both before surgery and at the last follow-up, are given in Table 1. Statistical comparisons between parameter values on the unaffected and affected sides are given in Table 2. Table 3 gives a comparison of parameter values according to the duration of dislocation and, Table 4 presents pre- and postoperative ROM measurements.
Before surgery, only one parameter (MUTA) was significantly different from the unaffected side in both AP and lateral views. PRUA and DRTA on the affected side were not significantly different from the unaffected side, while the other parameters were different in one view only (lateral or AP), not in both views.
At the last follow-up, two parameters concerning the proximal radius and ulna (PUTA and PRUA) were significantly different from the unaffected side in both AP and lateral views. MUTA, which had been significantly different between the affected and unaffected sides in both AP and lateral views before surgery, improved by the final follow-up, showing no side-to-side difference in the lateral view. For the other parameters, statistically significant changes were not noted in the comparison between affected and unaffected sides at the final follow-up.
Before surgery, only MRTA in AP view was significantly different between two groups of patients separated by duration of disease (Table 3). Comparison of ROM values before and after surgery (Table 4) showed decreased mean pronation and supination arcs after surgery, while the flexion-extension arc of the elbow was increased. After surgical reduction, two of the 22 patients (9%) had anterior subluxation of the radial head.
DISCUSSION
The nine parameters we measured on AP and lateral radiographs helped us to understand the changes of forearm bones following radial head dislocation. We found the MUTA to be significantly different in AP and lateral planes from the unaffected side before surgery, suggesting that the middle third of the ulna was mainly deformed (anteriorly in the lateral view and medially or laterally in the AP view). Similarly, Lincoln and Mubarak20) described an abnormal middle ulna in which the ulnar bow sign in the lateral radiograph occurred near the midpoint, at a mean distance of 45% ± 2% from the proximal end. We found an anterior ulnar bow sign on the affected side in 12 of 22 patients, while five patients showed no bow sign in both arms, and five showed it on both sides. Thus, the bow sign was only helpful in 54% of our cases.
At the last follow-up, the two parameters measuring the proximal radial and ulnar angles (PUTA and PRUA) were significantly different from the unaffected side in both the AP and lateral planes (Table 2). However, PUTA was different from the unaffected side only in the lateral view before surgery. PRUA was not different from the unaffected side preoperatively in either plane. We suspect this worsening is due to secondary deformation of the proximal radius and ulna because the radial head was reduced with a combined flexion osteotomy of the proximal ulna in some cases and annular ligament reconstruction. When the rotational axis of the two bones is not completely normalized after surgery, forearm rotation may be limited not only by remaining bony deformity. Excessive flexion osteotomy of the proximal ulna, aimed at placing the radial head in a correct position by tightening the interosseous membrane, can affect forearm rotation. An uncorrected proximal radial neck angle (PRTA) may also decrease forearm rotation.
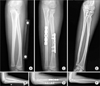
For a good result consisting of perfect reduction of the radial head and full ROM of the elbow and forearm, we believe that the surgeon must successfully correct all deformities (Fig. 4). However, this is not feasible in reality due to overlooked, overcorrected, and/or newly formed deformities after surgery. Based on our results, the middle of the ulna should be corrected in both AP and lateral views, but not with too much of a flexion component in the proximal ulna. Also, the PRTA should be carefully evaluated before surgery because a deformity there might go unrecognized and become a factor limiting forearm rotation when combined with a too-tightly reconstructed annular ligament. Rarely, the radial head may be stably reduced by corrective osteotomy alone in the ulna (the area of greatest deformity), and additional procedures (such as an annular ligament, etc.) may simply increase the risk of limited motion.
We found notching in the radial neck due to constriction by the reconstructed annular ligament in 13 of 22 cases. Because the triceps tendon has different elasticity from the original annular ligament, its greater constriction pressure may lead to notching in the neck during forceful rotation of the forearm, especially when the radial head is not rotated on the normal axis of rotation but instead is translated due to deformity. Similarly, the shape of the radial head also changed in eight of our 22 cases to adapt to the newly established radiocapitellar joint after surgery. Obviously, uncorrected deformities and/or deformity occurring after corrective osteotomy can lead to secondary deformity in this area.
Comparison of ROM before surgery and at the last follow-up (Table 3) showed decreased mean pronation and supination arcs, while the flexion-extension arc of the elbow was increased by reduction of the anteriorly dislocated radial head, which had been an obstacle for flexion and extension motion. The decreased arc of rotation again means that the deformities were not corrected sufficiently for the two bones to rotate normally. As Oka et al.21) described, little attention has been paid to morphologic features of the proximal radioulnar joint in chronic radial head dislocation because of the difficulties in evaluating them on plain radiographs. Tatebe et al.22) found a relation between PRTA and forearm rotation; the lesser the PRTA, the better the forearm rotation. Many studies indicate that the radial head becomes misshapen and overgrown within 3 years after injury and difficult to reduce.1117212324) However, the literature provides no clear guidance on what treatments may be required depending on the duration of dislocation or on the severity of deformity.
When we separated our patients by duration of dislocation of 4 months, we did not find any significant difference in parameters measured except in the middle radius. This result is difficult to explain. We certainly expect that the longer the duration of dislocation, the more severe the deformities should be. Our patients showed a wide range of duration of dislocation ranging from 1 to 96 months, with more procedures being required in the longer period cases. Two patients who had subluxation after reduction of the radial head had been untreated for 3 months and 96 months, respectively; the former had technical problems in the surgery and refracture at the osteotomy site by repeated trauma. However, other patients who were untreated for several years were successfully reduced.
We question, however, whether it would be possible to correct all deformities in actual surgery even if we did know everything about the existing deformities before the operation. We performed only one or two osteotomies in each bone of the forearm, which might not be sufficient in cases which have gone untreated for several years, especially those associated with deformities in the radial head and neck. For these, we need other procedures, including osteotomy in the proximal radius with shortening, radial head arthroplasty, and ulnar notchplasty to avoid impingement from the radial head. We can also add simultaneous rotation of the proximal part of the radius after the osteotomy, with angular correction and/or shortening to achieve more stable and congruent reduction. When the surgeon corrects the abnormal proximal radius, he or she should be very cautious to prevent nonunion or radioulnar synostosis.
The ROM of the forearm depends on many aspects of the bones and soft tissues,2526) but our radiographic study has not considered the latter. No matter how well the osteotomy sites are chosen, it is surely too much to expect that one or two osteotomies in the radius and/or ulna will suffice to restore normal anatomy and motion, especially in long-untreated cases including severe deformities. Our high success rate (91%) must be due to the various additional procedures18) which we performed.
We successfully reduced the dislocated radial head in 91% of our traumatic cases with a combination of many different procedures, in which the osteotomy sites were selected on the AP and lateral radiographs of the forearm. However, our patients showed decreased pronation and supination arcs after surgery, suggesting that uncorrected or newly developed deformities still remained, which was confirmed by our detailed analysis of patient radiographs.




 XML Download
XML Download