

 PDF
PDF ePub
ePub Citation
Citation Print
Print


As the population ages, the incidence of degenerative rotator cuff tears is on the rise and the tear sizes, known to grow with the patient's age, increase as well.1) Moreover the diagnosis of rotator cuff tears is becoming more prevalent due to technical advancements in radiological evaluation methods.2) In particular, for patients with greater than 5 cm retraction or full thickness tears of two or more tendons, concerted efforts are being made to improve the surgical techniques for arthroscopic rotator cuff repair in order to reduce their high retear rate which may reach 40%.3)
It is generally accepted that the excessive tension on the repaired footprint site is responsible for the high retear rate.4) Kim et al.4) showed that the tear size and tension at the repaired site were inversely correlated with healing. This also can be applied to irreparable rotator cuff tears that constitute up to 30% of all rotator cuff tears.5) Several studies have introduced techniques alterative to arthroscopic rotator cuff repair designed to augment or replace irreparable portions of the rotator cuff tendon and to reduce tension at the repaired site when it was impossible to reach the footprint area.67891011) Current scaffolds used for bridging or augmentation include the autogenic long head of biceps tendon (LHBT),12) allogenic or xenogenic patch grafts,78913) fascia lata autografts or allografts,8) and synthetic materials such as poly-L-lactic acid.14) Among them, allogenic and xenogenic patch grafts are receiving increasing attention and several surgeons have reported promising outcomes, such as functional improvement and satisfactory healing failure rates ranging from 8.3% to 27%.78) On the other hand, several other studies showed unsatisfactory results, including a 100% retear rate reported by Soler et al.13) Therefore, controversy still surrounds the functional and anatomical outcomes of the method. Similarly, the debate on the effectiveness of arthroscopic rotator cuff repair using the autogenic LHBT is ongoing. Ji et al.6) reported a 37% retear rate at 2 years postoperatively and Cho et al.12) showed a 75% retear rate in patients where the global fatty degeneration index (GFDI) of the supraspinatus, infraspinatus, and subscapularis was more than 2.0.
There are several reasons why individual outcomes differ markedly. First, the number of patients treated using the autogenic LHBT or allogenic dermal patch (ADP) is too small to draw meaningful conclusions. Second, the results are based on low levels of evidence, and few studies have compared the two different treatment options for irreparable rotator cuff tears. Thus, the purpose of this study was to compare outcomes and effectiveness of two different treatment options for bridging graft in irreparable massive rotator cuff tears by using an autogenic LHBT and an ADP. Furthermore, we investigated factors affecting the results of these two treatment methods. We retrospectively compared anatomic and functional outcomes of arthroscopic rotator cuff repair performed using the LHBT and ADP under the hypothesis that using LHBT would yield a higher healing rate in arthroscopic bridging for irreparable massive rotator cuff tears.
METHODS
Patient Enrollment
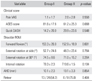
Between January 2011 and March 2015, 371 consecutive patients with massive rotator cuff tears were surgically treated at the Seoul National University Bundang Hospital. Data collection and all protocols were approved by the Institutional Review Board of Seoul National University Bundang Hospital (IRB No. B-1705-395-110) and performed in accordance with the principles of the Declaration of Helsinki. The informed consent was waived due to retrospective design of the study. Thirty-nine patients had massive rotator cuff tears evidenced by magnetic resonance imaging (MRI), which were unable to be mobilized and reattached to the footprint of the greater tuberosity due to considerable retraction of rotator cuff tendons. Among them, 29 patients had arthroscopic rotator cuff repair using the LHBT as the bridging graft. Five of these 29 patients were excluded from the analysis: four due to loss of follow-up and one due to considerable pain in the contralateral shoulder, which would affect postoperative rehabilitation highly dependent on the role of the opposite arm. Ten patients had arthroscopic rotator cuff repair using an ADP, and two of whom were excluded from the study: one due to loss of follow-up and the other due to previous surgery on the same shoulder that would affect final outcomes. Finally, a total of 32 patients were enrolled. In 24 patients, the LHBT was used as the bridging graft (group I). In the remaining eight patients, the LHBT was completely ruptured; thus, an ADP was used as the bridging graft (group II). In group I, there were 10 men and 14 women with a mean age of 66.9 years (range, 52 to 80 years), and their mean follow-up period was 14.5 months (range, 12 to 36 months). Of the 24 patients, eight patients had a partial tear of the LHBT; five patients had subluxation of the LHBT; and eight patients had a partial tear with subluxation. Three patients had type II superior labrum anterior to posterior (AP) lesions and the biceps tendon was tenotomized at the insertion site of the superior labrum. In group II, there were six men and two women with a mean age of 63.3 years (range, 53 to 77 years), and their mean follow-up period was 19.0 months (range, 14 to 60 months) (Table 1). In these patients, ADP grafts (MegaDerm, L&C Bio Co., Seoul, Korea; CGDerm, CGBio Co., Dae-woong Pharm, Seoul, Korea) were used for bridging the defect (Table 2). These grafts were chosen because (1) they were commercially available in Korea; (2) the companies produced thicker than 4 mm grafts; (3) it was difficult to obtain informed consent from patients on both the shoulder and thigh for using autologous fascia lata; and (4) reported outcomes of porcine dermis were poor13) and synthetic materials were not available to use in Korea. Nineteen patients in group I and four patients in group II had rotator cuff tears in the dominant hand.
For functional outcome assessment, the preoperative and final follow-up visual analogue scale (VAS) for pain, American Shoulder and Elbow Surgeons (ASES) score, and Quick Disabilities of the Arm, Shoulder, and Hand (DASH) score were evaluated. At the same time, active forward flexion (FF), external rotation (ER) at side, external rotation at 90°, and internal rotation (IR) behind the back were evaluated. For anatomical evaluation, fatty degeneration was evaluated preoperatively using the Goutallier classification by a blinded musculoskeletal radiologist who was not involved in the current study.15) Although we did not assess intraobserver or interobserver reliability of fatty degeneration of those muscles, we routinely evaluated all four rotator cuff muscles including teres minor1617) and interpretation was done by a senior radiologist who had experience of more than 10 years. Furthermore, the mean GFDI of the supraspinatus, infraspinatus, subscapularis, and teres minor was calculated. The AP dimension and medial retraction of the torn rotator cuff were measured with a probe with 5-mm markings (AR-10010; Arthrex, Naples, FL, USA) after debridement of the torn end. The healing failure rate was evaluated at 1 year after surgery using ultrasonography or MRI by a blinded musculoskeletal radiologist who was not involved in this study. Ultrasonography was used to evaluate rotator cuff integrity in patients who were not able to pay for MRI scans or had an MRI-unsafe device, such as a pacemaker. The acromiohumeral distance was calculated to see whether it was increased or maintained at the final follow-up.
Surgical Procedure
All surgical procedures were conducted by the senior author. The patient was placed in the lateral decubitus position under general anesthesia with traction of the involved arm. Using the posterior portal as the viewing portal, intra-articular pathologies, including biceps lesions, were evaluated. After glenohumeral inspection, subacromial decompression was performed, and acromioplasty was done if indicated. Then, the reparability of the torn rotator cuff was assessed and in cases where the torn tendon could not be attached even with medialization; an autogenic LHBT or ADP was used to bridge the defect.
For bridging with an autogenic LHBT, tenotomy was done at the insertion site of the biceps tendon to the superior labrum. After preparing the bleeding surface on the footprint, repair was done using two to three suture anchors. The first suture anchor was inserted at the anterior site of the prepared bone bed. One limb of the suture was inserted through the anterior site of the torn tendon while the rest of the suture was passed 2.5 cm distal to the tenotomized biceps tendon. The limb of the other suture anchors was additionally passed through the posterior retracted rotator cuff tendon at 1 cm interval, and matching sutures were passed through the LHBT. When the biceps tendon was interposed within the defect, knot tying was done to secure the biceps tendon (tenodesis) to the torn rotator cuff (Fig. 1).
For bridging with an ADP graft, the same procedure was performed to prepare the torn edge of the rotator cuff and bone bed at the greater tuberosity. The graft was cut to be 1–2 cm larger than the defect of the footprint at every border. Four to six different colored Fiberwire (Arthrex) were penetrated through the retracted rotator cuff tendon and only the threads that were located on the articular side were pulled through the lateral cannula. After piercing the patch with those threads at the matching site of the torn rotator cuff, the graft was introduced into the joint. Then, one thread from the rotator cuff and the other thread from the allogenic patch graft were retrieved and tied with the knot pusher sequentially. To reduce tension at the repaired site, suture anchors at the lateral border of the graft were occasionally inserted medial to the footprint and tied as in conventional single-row repair. If there were any sites requiring additional fixation, another Fiberwire was penetrated through the rotator cuff and allogenic patch by using a suture passer and firmly tied in a shuttle-relay manner (Fig. 2).
No passive shoulder motion was allowed during the 6 weeks after surgery. Active-assisted range of motion (ROM) was begun at 6 weeks after surgery. Muscle strengthening exercises were initiated at 3 months after surgery.
All statistical analyses were performed using IBM SPSS ver. 21.0 (IBM Corp., Armonk, NY, USA). The Mann-Whitney U-test was used to compare the two groups. The Wilcoxon signed-rank test was used to evaluate differences between the pre- and postoperative variables.
RESULTS
Functional Outcome
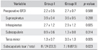
In group I, all functional scores significantly improved at the final follow-up (Table 3). Preoperative VAS for pain was 7.0 ± 2.5, decreasing postoperatively to 1.1 ± 1.7 (p < 0.001). The ASES score increased from 45.4 ± 19.1 to 81.6 ± 17.6 (p = 0.028) and the Quick DASH score improved from 50.0 ± 17.9 to 14.2 ± 20.0 (p = 0.017). In group II, preoperative VAS for pain was 5.9 ± 1.4, decreasing postoperatively to 2.0 ± 2.8 (p = 0.025). The ASES and Quick DASH scores were improved but without statistical significance (from 59.5 ± 33.5 to 61.2 ± 25.3 and from 43.9 ± 8.0 to 20.9 ± 23.6; p = 0.180 and p = 0.109, respectively).
At the final follow-up, group I showed better outcomes overall in terms of the VAS for pain, ASES, and Quick DASH scores. However, those scores did not show significant differences (p = 0.550, p = 0.068, and p = 0.548, respectively) (Table 4).
Range of Motion
In group I, ROMs improved (FF: 121.7° ± 46.9° to 153.3° ± 26.0°, p = 0.010; ER at side: 32.7° ± 21.0° to 52.7° ± 24.6°, p = 0.001; ER at 90°: 63.3° ± 20.1° to 74.5° ± 8.6°, p = 0.031; and IR: T10.5 ± 2.8 to T9.3 ± 2.3; p = 0.045). However, in group II, ROM increased but without reaching statistical significance (FF: 138.1° ± 36.6° to 152.9° ± 18.9°, p = 0.641; ER at side: 44.4° ± 21.9° to 48.3° ± 23.4°, p = 0.343; ER at 90°: 65.7° ± 19.0° to 71.0° ± 15.2°, p = 0.184 ; and IR, T11.5 ± 3.0 to T10.6 ± 1.5; p = 0.596, respectively) (Table 3).
At the final follow-up, group I showed better overall improvements in ROMs. However, there were no significant differences between the two groups (p = 0.601, p = 0.764, p = 0.264, and p = 0.104, respectively) (Table 4).
Anatomical Assessment
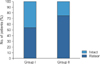
In group I, fatty degeneration was 3.9 ± 0.4 for the supraspinatus, 2.7 ± 1.2 for the infraspinatus, 0.9 ± 0.6 for the subscapularis, and 1.3 ± 0.7 for the teres minor. The GFDI was 2.2 ± 0.5 for the four muscles. A subscapularis tear was found in 8 out of 24 patients (33.3%). The tear size of retraction was 39.3 ± 6.1 mm and the AP dimension was 33.7 ± 8.3 mm. At 1 year after surgery, healing failure was found in 13 patients (54.2%) in group I (Fig. 3). In addition, more healing failure cases were found in patients with concomitant subscapularis tears (5 / 8 [62.5%] vs. 8 / 16 [50.0%], p = 0.238). In group II, fatty degeneration was 3.6 ± 0.5 for the supraspinatus, 2.9 ± 1.2 for the infraspinatus, 1.3 ± 0.8 for the subscapularis, and 3.0 ± 1.3 for the teres minor. The GFDI was 2.7 ± 0.7 for the four muscles. A subscapularis tear was found in seven out of eight patients (87.5%). The tear size of retraction was 39.4 ± 6.2 mm and the AP dimension was 38.5 ± 9.7 mm. At 1 year after surgery, healing failure was found in six patients (75.0%) in group II (Tables 1, 4, and 5, Fig. 3).
On intergroup comparison, fatty degeneration in the teres minor was worse in group II than group I (supraspinatus, infraspinatus, subscapularis, and teres minor: 3.9 ± 0.4 vs. 3.6 ± 0.5, 2.7 ± 1.2 vs. 2.9 ± 1.2, 0.9 ± 0.6 vs. 1.3 ± 0.8, 1.3 ± 0.7 vs. 3.0 ± 1.3; p = 0.288, p = 0.685, p = 0.314, and p = 0.005, respectively). Furthermore, a subscapularis tear was found in eight patients (33.3%) in group I and in seven patients (87.5%) in group II (p = 0.023). At 1 year after surgery, there were more cases of healing failure in group II than group I (13 / 24 [54.2%] vs. 6 / 8 [75.0%]; p = 0.404) (Table 4 and Fig. 3).
The acromiohumeral distance was significantly increased after surgery in both groups (Table 3). In group I, the acromiohumeral distance increased from 7.5 ± 1.5 mm before surgery to 10.1 ± 2.3 mm at the final follow-up (p = 0.006). In group II, the distance increased from 7.8 ± 2.8 mm before surgery to 10.1 ± 3.3 mm at the final follow-up (p = 0.046).
DISCUSSION
In spite of rapid improvement in medical devices and surgical techniques, surgical treatment of irreparable massive rotator cuff tears remains a challenge. This study showed unsatisfactory healing failure rates after bridging with autogenic LHBT (54.2%) or ADP (75.0%). In addition, patients receiving ADP grafts showed only relief of pain after surgery, and no significant clinical improvements were observed in various postoperative functional assessments.
In this study, we used ADP grafts because previous studies that involved the use of porcine dermis on the defect site showed high retear rates of the rotator cuff.1318) In addition, recent studies have revealed that the ADP graft is more effective than the xenogenic dermal patch graft. Ferguson et al.11) reported positive results of ADP grafts for augmentation in a meta-analysis where many studies described improved clinical condition with low retear rates. Moreover, they suggested that the xenogenic dermal patch graft should be used with caution since it has a high retear rate and may illicit inflammatory responses including infection. Interestingly, Ono et al.19) recently showed in a meta-analysis that bridging grafts had a higher healing rate than augmentation (77.9% vs. 64%). They conjectured that it could be because repair by bridging created less tension than augmentation over the repaired rotator cuff that was pulled excessively to the footprint area. However, Jones and Snyder20) reported a 41% of retear rate after bridging using an ADP. In addition, there are concerns over low mechanical properties of allogenic grafts compared to autogenic grafts and possibilities of inflammation due to DNA from an allogenic source.2122) Although it is difficult to draw a definite conclusion because of the lack of previous studies and the small sample size in our study, the effectiveness of the ADP graft is questionable, considering that it had a 75% of retear rate and did not show significant improvement in function (except for pain relief) and ROM.
It is true that the type of graft is important. However, since many studies reported that the retear rate increases with severe fatty degeneration and most massive rotator cuff tears are accompanied by chronic fatty degeneration,3) the severity of fatty degeneration should be considered when graft is used.23) In a study by Gupta et al.,7) the retear rate was only 20%–24% when ADP grafts were used for selected patients with low fatty degeneration. Moreover, Mori et al.8) performed rotator cuff repairs using autogenic fascia lata and reported that 8.3% of patients showed retears at the final follow-up. However, this study also included patients with grade one or two fatty degeneration in the infraspinatus according to the Goutallier classification, which was a limitation. When the same authors23) investigated the healing failure rate in patients with high fatty degeneration, the retear rate was 89.4%, indicating that this approach was not suitable in cases with high grades of fatty degeneration. Considering the results of those studies, we think that the high healing failure rate (75%) in group II could be attributable to the fact the patients had a mean GFDI of 2.7.
In our study, the degree of fatty degeneration in the teres minor was higher in the group receiving ADP grafts than the group receiving an autogenic LHBT graft (p = 0.005). Recent studies on rotator cuff repair have highlighted the impact of fatty degeneration of the teres minor. The teres minor contributes to the function of shoulder where it is responsible for 3% of adduction, 16% of extension, and 14% of external rotation of the shoulder joint.24) Moreover, since only the teres minor can roll as the external rotator in the case of massive rotator cuff tears, including supraspinatus and infraspinatus tears, it can be considered to contribute significantly to the range of shoulder joint movement.25) Although we are not aware of any studies evaluating the effects of the teres minor on healing failure in rotator cuff repair, a previous study26) reported that patients with higher fatty degeneration of the teres minor that received a reverse total shoulder arthroplasty had less desirable clinical results. Therefore, extensive fatty degeneration of the teres minor may have affected the clinical and anatomic outcomes in our study.
In this study, seven out of eight patients who underwent repair with ADP had subscapularis tears. Therefore, subscapularis tears could be one of the factors affecting the rate of healing failure in grafted tissue. A previous study reported that 69% of large or massive tears were accompanied by subscapularis tears and many of these had concomitant complete rupture of the LHBT.27) Park et al.28) showed that among patients who underwent arthroscopic repair for posterosuperior rotator cuff tears, patients with more than 50% of their subscapularis torn had a 43% retear rate, which was higher than in patients with less than 50% tears or no tears. Moreover, large subscapularis tears highlight the underlying decreases in both the cellularity of fibroblasts and the number of blood vessels that inhibit the healing capacity of a tissue.29) These mechanisms may be responsible for the high rate of healing failure in this study.
Compared to the healing failure rates documented in previous studies (36%–41.7%),1012) group I showed a relatively high rate of 54.2%. As stated above, this could be due to the GFDI being higher than 2.0. However, compared to group II, group I had a low healing failure rate, which may be associated with the fact that the degree of fatty degeneration of the teres minor was lower than that in group II and only 8 out of 24 cases had accompanying subscapularis tears (33.3%) unlike in group II where all patients except one had subscapularis tears (87.5%). In addition, since the “autogenic" LHBT was used instead of an allogenic source, the immune response may have been less severe30) ultimately affecting the clinical and anatomic outcome. There have been few studies that involved the use of an autogenic LHBT. Ji et al.6) restored irreparable U-shaped rotator cuff tears by using the LHBT without cutting it off from the attachment to the labrum and reported a retear rate of 37% at 2 years after operation. Moreover, Rhee et al.10) performed bridging by using open or arthroscopic autogenic LHBT grafts and reported a 64.3% healing rate. They concluded that it could be useful to restore the torn rotator cuff, which is hard to pull to the original position. However, they also reported in another study a 75% retear rate when the GFDI was higher than 2.12) Thus, the outcomes of this technique are still controversial.
Despite the relatively high healing failure rate, the final mean acromiohumeral distance increased by 2.6 mm and 2.3 mm in group I and group II, respectively. Our results agreed with a previous multivariate analysis study on 108 patients who underwent arthroscopic rotator cuff repair for massive rotator cuff tears where the decrease in postoperative acromiohumeral distance was considered the only factor suitable for determining functional deterioration. In spite of severe anatomical failure, the postoperative maintenance and increase of acromiohumeral distance can lead to an improvement in pain and function as in group I and pain relief as in group II because force coupling was maintained to some degree.
There are several limitations to this study. First, the number of patients was small increasing the probability of beta error. However, it was practically impossible to enroll sufficient subjects due to the lack of patients with irreparable rotator cuff tears even by the large-volume surgeons. Furthermore, in spite of the small number of patients, the significance of this study lies in the fact that this was the first study to compare the outcomes of two different methods of bridging graft, which would be beneficial for surgeons in determining a treatment strategy. Second, different types of ADP grafts were used in group II, and such heterogeneity could have affected the outcome. Moreover, selection bias could not be ruled out. Group I received a LHBT graft when available and only 8 out of 24 cases were accompanied by subscapular tears, whereas group II had completely ruptured LHBTs and seven out of eight cases were accompanied by subscapular tears. In addition, group II showed higher fatty degeneration in the teres minor. These factors may have resulted in worse clinical or radiological outcomes in group II irrespective of the difference in graft material. Lastly, the short follow-up period was an additional limitation.
In this study, both groups showed maintenance or increase in the acromiohumeral distance at the final follow-up. All functional scores, including VAS, improved in group I although VAS decreased significantly in group II. Considering these results, it can be assumed that bridging grafts are effective in maintaining force coupling of the rotator cuff. However, both groups showed high healing failure rates and most patients in group II had healing failure. In addition, in contrast to group I, no significant improvements were observed in group II, except for pain VAS. Therefore, the surgeon should carefully consider the surgical options for irreparable massive rotator cuff tears, especially in patients with severe fatty degeneration in the teres minor or combined biceps and subscapularis tears.





 XML Download
XML Download