

 PDF
PDF ePub
ePub Citation
Citation Print
Print


One of the important factors that affects the long-term survivorship of total knee arthroplasty (TKA) is the postoperative limb alignment.12) Increased incidence of aseptic loosening has been reported in patients with persistent abnormalities in the mechanical axis following TKA.34) A coronal plane valgus orientation lying between 2.4° and 7.2° is regarded as the ideal postoperative alignment of TKA.4) The initial varus position of the TKA implant is expected to worsen with time, probably due to abnormal polyethylene wear in the medial compartment.5)
There is a relatively high incidence of tibial and femoral deformity in Asian patients with osteoarthritis of the knee (Fig. 1).6) Lateral tibia vara and varus orientation of the joint line are not infrequent in Asian patients undergoing TKA.67) Varus tibial alignment was associated with a 3.2 times greater risk of failure of TKA in a study by Fang et al.3)
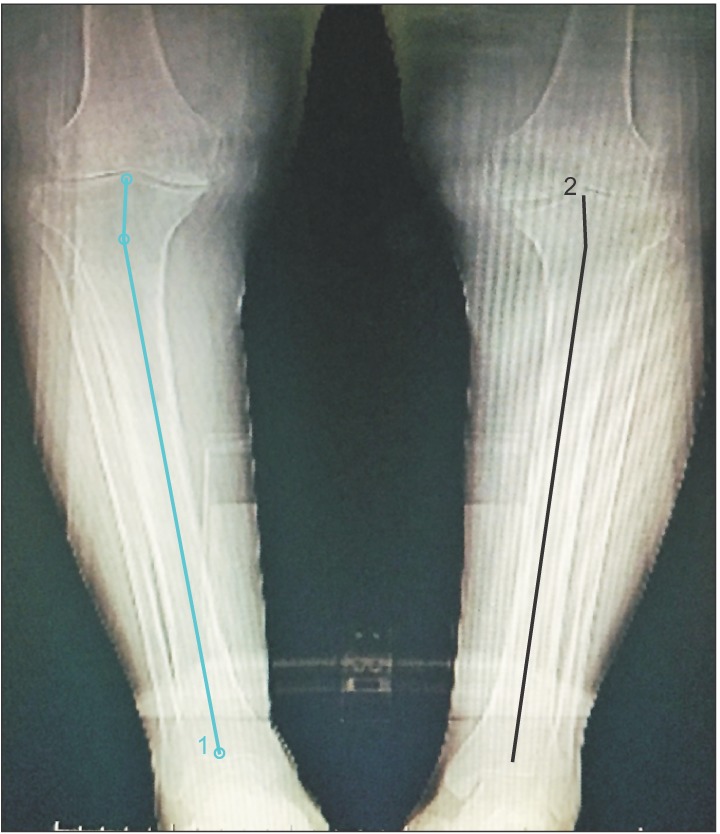 | Fig. 1Preoperative scanogram showing bilateral osteoarthritis of the knees with proximal tibia vara. The longer line represents the anatomical axis of the tibia. The shorter line is drawn from the center of the line along the tibial plateau and perpendicular to the plateau. The angle between the two lines is the magnitude of proximal tibia vara.
|
Extramedullary tibial guides are preferred by most surgeons for alignment of the tibial component in TKA. When using extramedullary guide, the center of the intercondylar eminence has been the standard proximal reference point for the tibial plateau. However, it has been observed that the tibial cut referenced to the center of the intercondylar eminence leads to a varus malalignment in the presence of preexisting proximal tibia vara.89)
The purpose of this study was to investigate whether lateralization of the lateral tibial plateau reference point (based on the magnitude of proximal tibia vara) contributes to optimal postoperative coronal plane alignment of the total knee prosthesis. We hypothesized that in TKA in patients with proximal tibial vara, acceptable degree of accuracy can be achieved with the use of extramedullary jig for tibial component alignment by lateralizing the reference point.
METHODS
This was a prospective study involving pre- and postoperative evaluation of coronal plane profile of the lower limbs in patients with proximal tibia vara who underwent TKA. The study was approved by the Hosmat Ethics Committee (HEC/2012/045). Informed consent was obtained from all the participants. Patients undergoing primary TKA for osteoarthritis of the knee with coronal plane tibia vara were included in the study. Patients with posttraumatic knee arthritis, deformities of tibia due to old fractures and patients undergoing revision knee arthroplasties were excluded from the study. A total of 214 TKA procedures were performed in 163 patients between June 2012 and July 2014. PFC Sigma (Depuy/Johnson and Johnson, Warsaw, IN, USA) implants were used in all the patients. The mean follow-up period was 3.4 years and minimum follow-up period was 2 years. No patient was lost to follow up. Kellgren-Lawrence grading was used to assess the severity of osteoarthritis.10)
Pre- and postoperative evaluation consisted of standing X-ray scanogram with the lower limb in 15° of internal rotation with the patellae facing forward (Fig. 1). The following measurements were performed—mechanical axis deviation, degree of tibia vara, proximal lateral reference point of tibial condyle, and coronal alignment of femoral and tibial components. The measurements were performed using the DICOM software (Kriens, Switzerland). Three surgeons (RKT, MNK, and RS) performed the measurements independently and the average of the three measurements was obtained. Intraclass correlation ratings were calculated to assess interobserver reliability. Tibia vara was measured as described earlier by Yau et al.6) From the preoperative scanograms, the lateral reference point of proximal tibia was determined. The distance between the center of the intercondylar eminence and the lateral condyle reference point was calculated. The same reference point was replicated intraoperatively (Fig. 2). For the purpose of this study, we defined proximal tibia vara as a minimum of 5° of coronal plane angulation. The deformity was considered as laterally angulated tibia vara if the distal axis angulated towards the midline and medially angulated tibia vara if the distal axis angulated away from the midline.6)
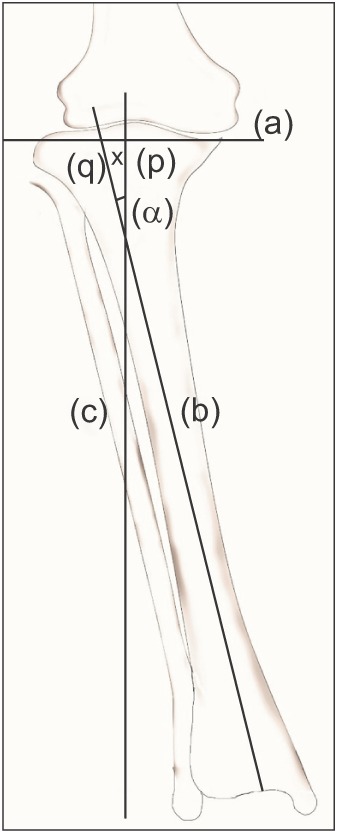 | Fig. 2Diagrammatic representation of the method of determining the lateral tibial reference point. (a): Line drawn along the tibial articular surface, (b): line drawn along the anatomical axis of the tibia, (c): line drawn perpendicular to line (a) at the center of the tibial intercondylar eminence, (p): center of the intercondylar eminence, (q): point of intersection of lines (a) and (b), angle α: angle between lines (b) and (c), x: distance of the reference point from (p).
|
During the operation, the knee joint was exposed through the medial parapatellar approach and the patella was everted. The soft tissues at the anterior edge of the lateral tibial condyle were cleared to allow placement of the jig firmly against the bone (Fig. 3). Adequate clearance of the soft tissues anterior to the paracentral area of the lateral condyle is very important for allowing lateral placement of the jig. The tibial reference point was measured from the center of the intercondylar eminence and marked using a marking pen (Fig. 4). The extramedullary jig was placed so that the reference marking on the jig was colinear with the reference line marked on the lateral tibial plateau (Fig. 5). The jig was affixed to the tibia using the lateral pin. The lower end of the jig was placed at the center of the ankle (Fig. 6). The coronal alignment was then checked using the alignment rod (Fig. 7). The medial pin was then used to fix the jig to the medial tibial condyle. This was followed by tibial resection.
 | Fig. 3Extent of exposure of the lateral tibial condyle required for correct placement of the extramedullary jig.
|
 | Fig. 4Intraoperative photograph showing the lateral condylar reference line which is 10 mm lateral to the center of the intercondylar eminence.
|



Magnitude of lateralization of the tibial plateau reference point (and its relation to the magnitude of proximal tibia vara), postoperative mechanical axis, tibiofemoral angle and medial tibial and femoral component angles were the primary variables. Clinical outcomes of pain and knee function were secondary variables. Linear regression analysis was used to assess the relationship between tibia vara and lateralization of the proximal tibia reference point from the center of intercondylar eminence. The R2 value and p-value were calculated. Postoperative outcome assessment was performed using the Knee Society Score (KSS).11) The Student t-test was used to test the significance of difference between pre- and postoperative outcome scores (pain score and function score) and a p-value less than 0.05 was considered as significant. Statistical analysis was carried out with the aid of the SPSS ver. 17.0 (SPSS Inc., Chicago, IL, USA).
Go to : 
RESULTS
Sixty-two patients (95 knees) with proximal tibia vara (coronal angulation of tibia more than 5°) were enrolled in this study. The descriptive statistics of the patient cohort involved in the study are shown in Table 1 and the radiographic measurements are summarized in Table 2. The intraclass correlation for interobserver variation in the preoperative measurement of tibia vara was 0.86 (95% CI, –0.90 to 0.93; p < 0.01). The proximal tibial reference point (as determined from the preoperative scanograms) was lateral to the center of the intercondylar eminence by a mean 7 mm (standard deviation [SD], 2.2 mm). Postoperatively the tibiofemoral angle was 6° to 10° of valgus in 94% of cases. There was no lateral overhang of the tibial implant in any of the patients. The coronal plane orientations of tibial and femoral implants were within acceptable limits. Linear regression analysis showed a very high degree of positive correlation between the magnitude of tibia vara and the amount of lateralization of the tibial reference point (R2 = 0.79, p < 0.001) (Fig. 8).
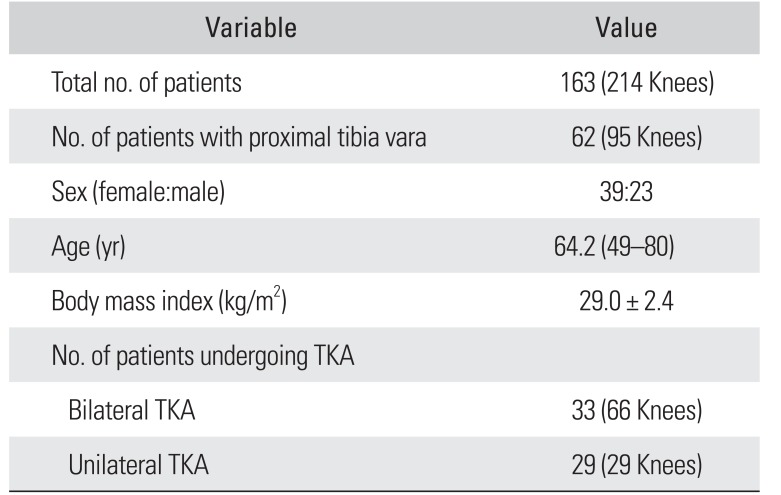
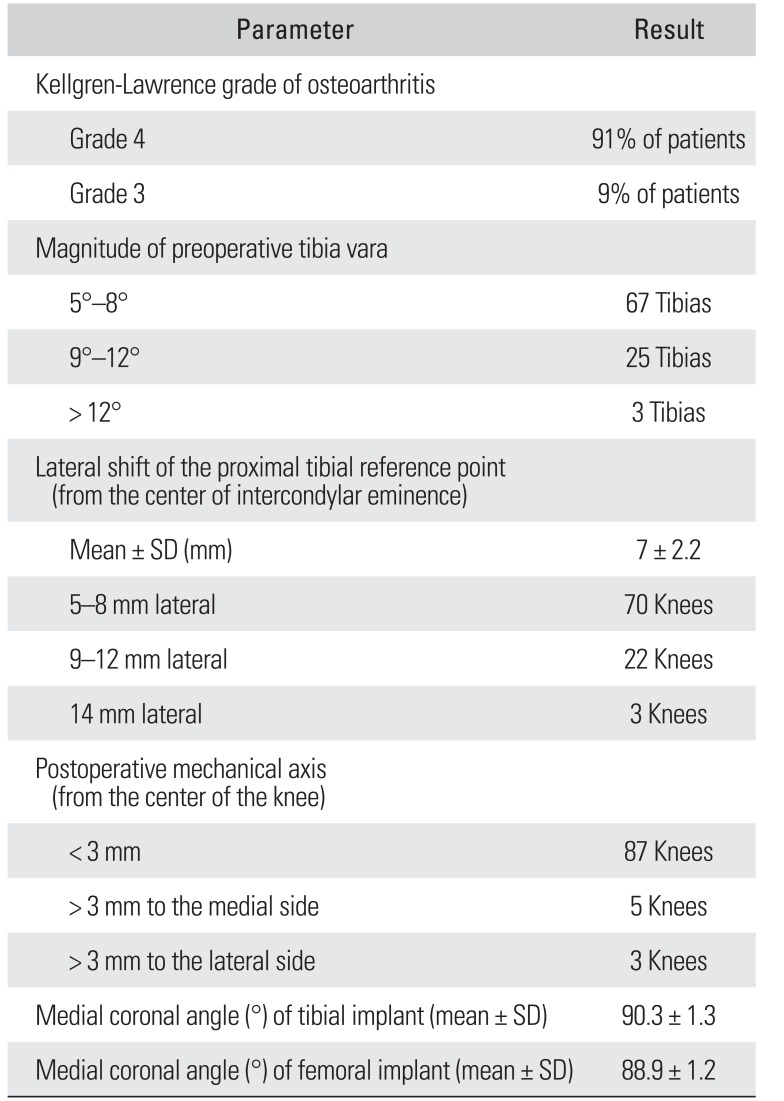
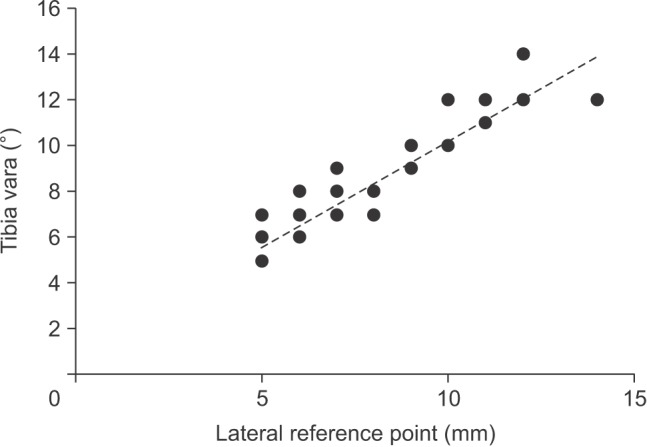
Table 1
Descriptive Statistics of the Patient Cohort
![]()
Table 2
Summary of the Radiographic Measurements
![]()
The mean preoperative KSS was 27.4 (SD, 8.7) and functional score 26.5 (SD, 9.6). Postoperative mean knee pain score was 96.3 (SD, 6.6) and functional score was 94.9 (SD, 6.1) and the difference was significant (p < 0.001) in both pain and function scores.
Go to :
DISCUSSION
Intramedullary alignment has been reported to be more accurate than extramedullary guides in studies involving Caucasian populations with relatively straight tibias.12131415) However, it is less accurate in the presence of coronal plane deformities of the tibial shaft.816) Severe deformities may preclude the passage of the intramedullary alignment rod down the entire length of the tibial shaft.14) Short intramedullary rods have been considered adequate in tibias with nondeformed shafts but are not realistic in tibia vara.17) Extramedullary guides are useful even in the presence of tibia vara and they potentially minimize the risk of fat embolism, intraoperative fracture, loss of bone cement pressurization and iatrogenic fracture in the presence of cortical bone pathology.18)
While extramedullary tibial guides are advantageous, correct positioning of the extramedullary jig is vital to minimize errors in alignment.1618192021) The efficacy of computer or robotics assisted TKA and patient specific instrumentation in knees with tibia vara has not been supported by existing literature.2223242526) It is tempting to resect larger amounts of lateral tibial plateau for achieving proper orientation of the TKA but unduly large resection can lead to subsidence of the implant.27)
In Asian patients with varus osteoarthritis, the center of the tibial plateau is often medial to the anatomic axis (center of the tibial shaft). Thus, it is not an ideal reference point for the placement of the tibial component.28) Earlier studies have recommended the use of lateral edge of intercondylar eminence instead of center of intercondylar eminence as the reference point.89) In our study, we have not used the lateral intercondylar eminence as a fixed reference point. The reference point was individualized based on the degree of metaphyseal tibial deformity and it can extend even further lateral to the lateral intercondylar eminence. This is illustrated in Fig. 9A which shows a persistently varus tibial component angle (87.7°) in the left knee of a patient with tibia vara who underwent bilateral TKA. The left TKA had been performed earlier to this study using the center of the tibial plateau as the entry point. The right TKA in the same patient (Fig. 9B) was performed few months later using the lateral tibial plateau entry point and the tibial component angle was more satisfactory (90.4°).
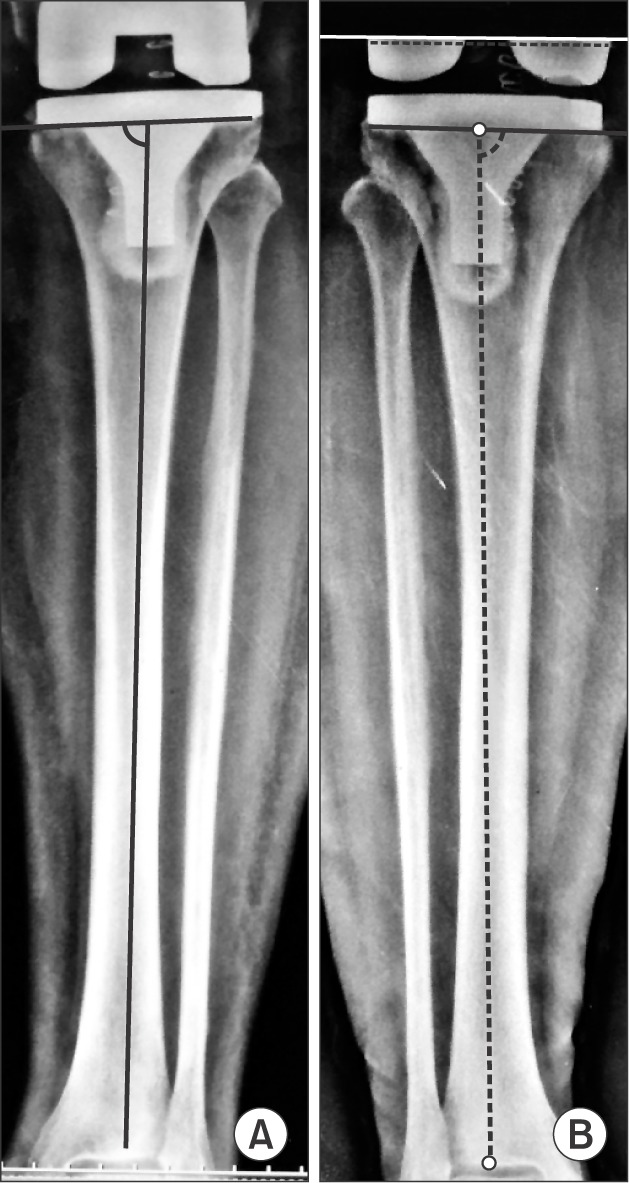 | Fig. 9(A) Postoperative radiograph showing suboptimal medial component angle of 87.7° with the use of the central intercondylar reference point in a patient with proximal tibia vara. (B) Postoperative radiograph showing medial tibial component angle of 90.4° obtained using the lateral tibial condylar reference point in the contralateral knee of the same patient.
|
There are limitations to this study. It is performed on Asian patients and the anatomical characteristics of the involved bones may be different in patients of other ethnicities. The study does not prove that improvement of accuracy of coronal plane alignment by this technique of lateralized reference point leads to improved longevity of the implant. Long-term survivorship studies are essential for this.
During TKA in patients with proximal tibia vara, reasonable degree of accuracy can be achieved with the use of extramedullary jig for tibial component alignment by lateralizing the proximal tibial reference point. We recommend that the degree of lateralization should be individualized based on the deformity on preoperative full-length radiographs.
Go to :
 XML Download
XML Download