

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Unicompartmental knee arthroplasty (UKA) is an established option for surgical treatment of isolated osteoarthritis within one of the three compartments of the knee joint.1) In recent years, UKA has gained popularity amongst surgeons and patients alike as its mid- and longterm results are encouraging.2) The current literature shows that the first-decade survivorship after UKA has been improved and is comparable with that of total knee arthroplasty (TKA) in patients aged more than 60 years.3) UKA offers several advantages over TKA in that (1) the surgery is less invasive; (2) patients tend to have their knee flexion preserved; and (3) the operated knee retains much of its biomechanics leaving patients to have a normal feeling knee.2) Longo et al.4) in their systemic review have advocated the routine use of UKA for medial compartment osteoarthritis.
While UKA has advantages over TKA, national joint registries report a significantly higher revision rate of UKA.5) As a result, most surgeons are highly selective, offering UKA only to a small proportion of patients requiring arthroplasty of the knee and consequently performing only a few UKA procedures each year. This is likely to be perpetuated by the fear of poor outcomes following UKA. The overall size of the practice is often beyond the surgeon's control. Therefore, the case volume may only be increased by broadening the indications for surgery and offering UKA to a greater proportion of patients requiring arthroplasty of the knee. However, this must be balanced against appropriate care for the patient.
Appropriate care is defined as care that is associated with the net clinical benefit to the patient.6) There is still a lot of controversy regarding the sweet spot with respect to the preoperative scores and symptom levels that are associated with the likelihood of good outcome following medial UKA and the influence of patient demographics on these. In this study, we also questioned given that indications for medial UKA are met, whether there are optimal predictors of a good outcome defined as clinically important improvement in outcome scores following UKA in an Asian population.
The purpose of this study was to evaluate predictors of good outcomes following medial UKA in Asian patients. We hypothesized that age and preoperative kneespecific scores would be optimal predictors.
METHODS
Study Sample
Institutional Review Board of Singapore Health Services (SingHealth) granted a waiver for this study as no patient identifiable data was used. Prospective registry data of all primary unilateral medial UKAs performed at Singapore General Hospital between January 2006 and December 2011 were collected. Patients were included only if they underwent a primary unilateral medial UKA with the other knee asymptomatic or successfully replaced and completed all appropriate follow-up appointments and outcome assessments. Exclusion criteria were as follows: (1) spastic or flaccid paralysis of one or both lower limbs regardless of cause, (2) New York Heart Association Class II and III cardiac failure,7) (3) severe pulmonary disorders limiting the patient to only home ambulation, (4) all revision arthroplasties including infected arthroplasties, and (5) lateral UKAs. There were only 10 lateral UKAs in the registry and these were excluded for ease of interpretation of mechanical alignment pre- and postoperatively.
Perioperative Details
All medial UKAs were performed for medial noninflammatory primary osteoarthritis of the knee. UKAs were only performed in knees with an intact contralateral compartment and patellofemoral changes not greater than grade II or III (Ahlback classification). Trochlear wear up to grade IV was accepted if the distribution of wear was central. All UKAs were preformed by fellowship-trained surgeons in adult reconstruction. Anaesthesia was either general or spinal with some patients receiving a femoral nerve block perioperatively as a single bolus. Each operation was performed with a tourniquet except in vasculopathic patients, and all patients were given a single injection of intravenous prophylactic antibiotic just before skin incision (cefazolin or vancomycin if the patient was allergic to penicillin). A midline skin incision or a medially skewed longitudinal incision was made, and the joint was exposed through a medial parapatellar arthrotomy. An anteromedial wear pattern on the tibia was used as a surrogate for a competent anterior cruciate ligament. All implants used were of fixed-bearing design: M/G UKA from Zimmer (Warsaw, IN, USA) and PFC UKA from Depuy (Warsaw, IN, USA). Antibiotic-impregnated cement was used in all patients. Postoperatively, all patients were part of a coordinated clinical care pathway. All patients received mechanical and oral prophylaxis against venous thromboembolism. They were assessed by a physiotherapist daily, and ambulation was initiated as soon as the patient was able to perform a straight-leg raise actively. Patients were discharged when they were able to ambulate at least 20 m independently with or without a walking aid and able to climb stairs. Patients were either discharged directly to their homes or to a rehabilitative facility. They were then followed up at the specialist outpatient clinic at 1 month, 3 months, 6 months, 1 year, 2 years, and 5 years postoperatively.
Assessments
All assessments were completed independently at the Orthopaedic Diagnostic Centre of our institution. Baseline interviews were conducted preoperatively to assess sociodemographic characteristics, body mass index (BMI) and knee arthritis severity, using the Oxford Knee Score (OKS),8) for which higher scores indicate greater severity, the Short Form 36 (SF-36) questionnaire9) and the Knee Society Score (KSS).10) For the purposes of this study, we chose to assess outcomes using only the Physical Component Score (PCS) and the OKS because the Mental Component Score (MCS) of the SF-36 questionnaire has been shown to have poor correlation and wide variability in Asian populations.11) Furthermore, there has been no validated minimal clinically important difference (MCID) for the MCS and KSS. Comorbidities were assessed via the electronic health records at our institution. Alignment was measured on the lower limb long leg radiographs obtained pre- and postoperatively. Varus was considered positive and valgus negative in the analyses.
Definition of Good Outcome
In the absence of universally accepted criteria, our primary analysis defined a good UKA outcome as an overall improvement in the outcome scores greater than or equal to the MCID. This was the same definition used by Hawker et al.12) in their study of predictors in patients undergoing total joint arthroplasty. The MCID represented one-half of the standard deviation of the difference between the preand postoperative outcome scores.13) The calculated MCID for our cohort of patients was 5 for the OKS and 10 for the PCS.
Statistical Analysis
Clinical variables were used to develop a multiple logistic regression model for good UKA outcomes at 5 years postoperatively through a stepwise variable selection model building approach using the Akaike Information Criterion. 14) The continuous variables considered in this model include age, BMI, preoperative flexion range, preoperative KSS, preoperative OKS, preoperative MCS, preoperative PCS and preoperative mechanical alignment. The categorical variables considered in this model include gender, education, race, operated side, and number of comorbidities. The likelihood ratio test was used to determine the pvalues of the variables that entered the model. Finally, the odds ratio for a good outcome (MCID criterion) associated with each of the identified predictors was determined using log Poisson regression. All p-values less than 0.05 were considered significant. All statistical analyses were performed using SAS ver. 9.3 (SAS Inc., Cary, NC, USA).
RESULTS
Preoperative Characteristics of Patients
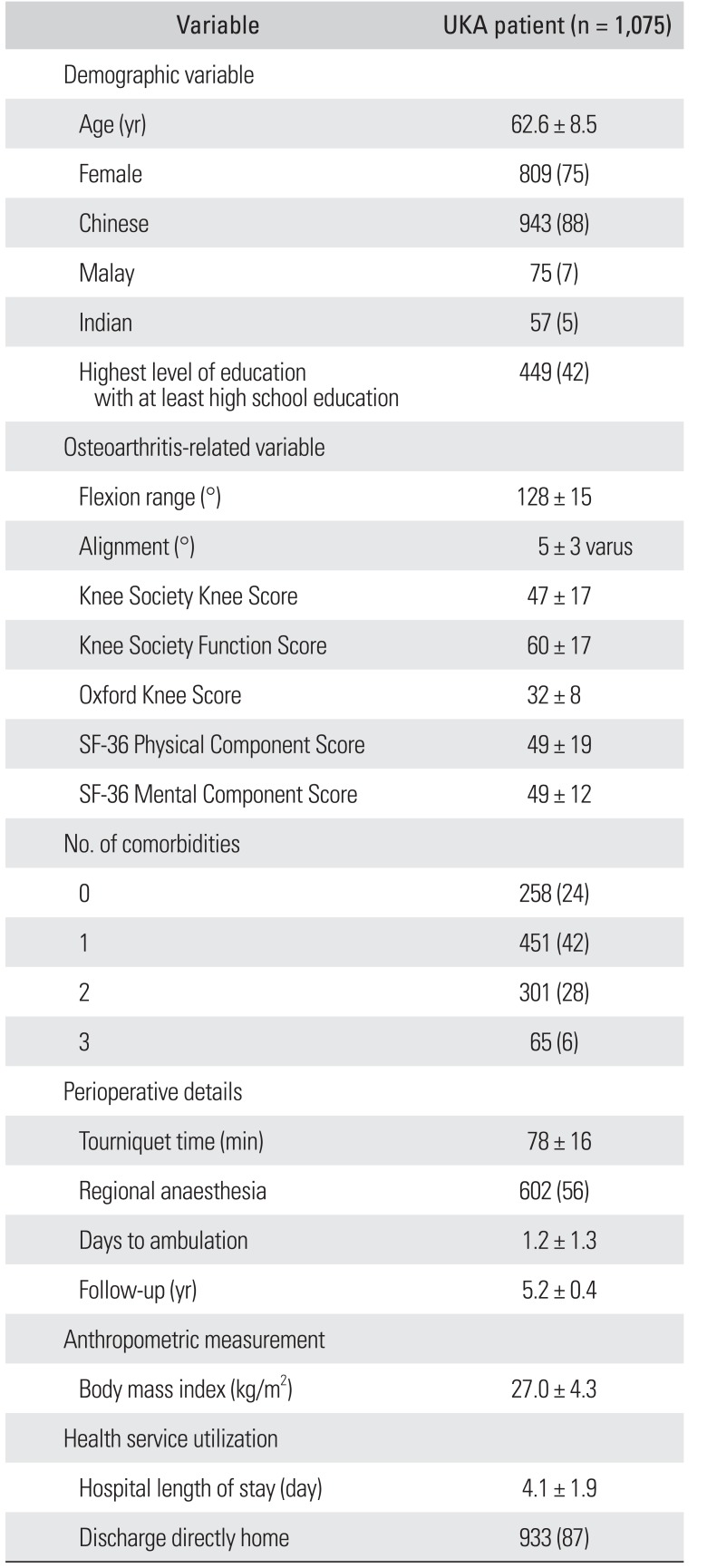
There was a 3% loss to follow-up rate. A total of 1,075 patients with a mean follow-up of 5.2 years were available for final analysis. Clinical details of the 1,075 patients are shown in Table 1.
Postoperative Outcomes of Patients
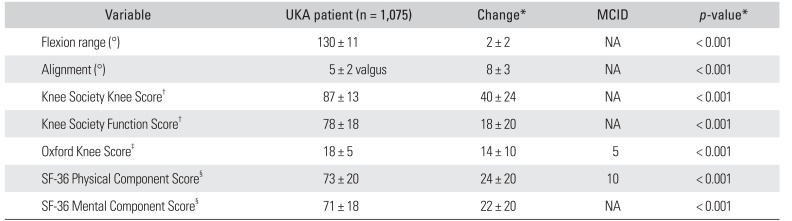
Patients significantly improved in all objective and patientreported outcomes 5 years following medial UKA as reported in Table 2. The mean flexion improved from 128° to 130° (p < 0.001). The mean mechanical alignment improved from 5° varus to 5° valgus (p < 0.001). The mean Knee Society Knee Score (KSKS) improved from 47 to 87 (p < 0.001). The mean Knee Society Function Score (KSFS) improved from 60 to 78 (p < 0.001). The OKS improved from 32 to 18 (p < 0.001). The SF-36 PCS improved from 49 to 73 (p < 0.001). The SF-36 PCS improved from 49 to 73 (p < 0.001). The SF-36 MCS improved from 49 to 71 (p < 0.001).
Predictors of Good Outcome Following Primary Medial UKA
Our primary analysis modelled predictors of good outcome following primary medial UKA using the MCID criterion (Table 3). When a good outcome was defined as achievement of the MCID for the OKS, only preoperative OKS was found to be an optimal predictor. For every 1-point increase (worsening) in the preoperative OKS, patients were 1.27 times more likely to report a good outcome. When a good outcome was defined as achievement of the MCID for the SF-36 PCS, only preoperative SF-36 PCS was found to be an optimal predictor. For every 1-point decrease (worsening) in the preoperative SF-36 PCS, patients were 1.08 times more likely to report a good outcome. When a good outcome was defined as achievement of the MCID for both the OKS and SF-36 PCS, preoperative KSKS and preoperative SF-36 MCS were found to be optimal predictors. For every 1-point decrease (worsening) in the preoperative KSKS and 1-point increase (improvement) in the preoperative SF-36 MCS, patients were 1.02 times more likely to report a good outcome. Secondary analyses revealed that 88% of our patients experienced a good outcome at 5 years based on OKS and 74% did based on PCS.
DISCUSSION
Western studies have showed that better patient selection has improved satisfaction rates and implant survival following medial UKA. This study aimed to evaluate predictors of outcomes after medial UKA in Asians. The most important findings of our study are that we found a majority of Asians achieving a good outcome following medial UKA and that preoperative OKS, KSKS, and SF-36 scores were optimal predictors of 5-year outcomes following the index surgery.1516)
By our definition of good outcome using the MCID criterion, a majority of our patients undergoing medial UKA experienced a clinically significant improvement in their functional outcomes following surgery. Four functional outcome measures had good potential for predicting clinically significant improvement in outcomes based on the OKS and the PCS. These were the preoperative OKS, SF-36 PCS, KSKS, and SF-36 MCS.
The KSS, SF-36, and OKS have all been validated and are both responsive and reproducible, henceforth the choice of these scoring systems in our study. Parratte et al.17) found improvements in both the KSKS and KSFS in mobile and fixed bearing UKAs at a mean follow-up duration of 15 years. Improvement was also seen in the range of motion from a mean flexion of 120° to 129°. Similar findings were also seen by Li et al.18) when they compared the KSKS and KSFS for mobile and fixed bearing UKAs at a mean follow-up period of 31.9 months. In a series of 150 patients, Jahromi et al.19) found the mean OKS to be 22.17 at a minimum follow-up period of 12 months. There were no preoperative OKS to compare to in this series but they found that the ability to kneel and then stand up was significantly worse than scores for other aspects of the OKS. Another study of 260 patients who underwent UKA showed an improvement of the OKS from a mean of 24 to 40 at 1-year postoperative period.20) Zuiderbaan et al.21) found that, at a minimum of 2-year follow-up, all 104 patients in their series showed improvement in all domains of the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) score. Similar findings are seen in our study with respect to patient reported outcome measures. However, the improvement in range of motion in our patients was less marked than in Western literature. This may be due to the good flexion range in our patients preoperatively.
The initial early results of UKA were discouraging with failure rates reported as high as 30%.22) Kozinn and Scott23) defined a set of criteria for the ideal medial UKA candidate: (1) low functional demand, (2) age > 60 years, (3) weight < 90 kg, (5) minimal pain at rest, (6) flexion contracture less than 5°, and (7) a passively correctable angular deformity. Since then, several other authors have gone on to identify factors that predict for both good and poor outcomes.2425) Our study found that preoperative OKS, KSKS, SF-36 PCS, and MCS were predictive of a good outcome following medial UKA as defined by achievement of the MCID for OKS and/or SF-36 PCS. These findings are mirrored by similar studies in the Western literature. Munk et al.20) conducted a review of 260 patients at 1-year postoperative interval and found that baseline OKS was a predictor of outcomes. Outcomes evaluated in their study were the OKS, global patient satisfaction, and global patient result. Thus far, there have been no studies that have reported preoperative SF-36 PCS and KSKS as optimal predictors of a good outcome following medial UKA. The SF-36 PCS consists of the following domains: (1) general health, (2) physical functioning, (3) role-physical, and (4) bodily pain. The KSKS is an objective score that has the following domains: (1) alignment, (2) instability, (3) joint motion, and (4) symptoms. Our study indicates that patients with poorer preoperative general physical condition as well as poorer knee function have a higher likelihood of obtaining a good outcome following medial UKA. While there are two studies that found a similar trend in subsets of TKA patients, we found no study that reported the predictive value of the SF-36 PCS and KSS from UKA registry data.2627)
Interestingly, we found that preoperative SF-36 MCS is a significant predictor of good outcome following medial UKA. The SF-36 PCS consists of the following domains: (1) role-emotional, (2) vitality, (3) mental health, and (4) social functioning. Our study suggests that patients with a better preoperative general mental condition have a higher likelihood of having a good outcome following medial UKA. This has been mirrored by Lee et al.28) in their study evaluating predictors of satisfaction with UKA in an Asian population. They investigated dissatisfaction rates in 724 UKAs and reported that poorer preoperative SF-36 MCS was associated with patient dissatisfaction at 2 years following UKA.
There are variables that were found not to be significant predictors in our study contrary to the reports in the literature. The scope of our study did not include evaluation of preoperative radiographic findings. However, Munk et al.20) did report that lateral subluxation of the patella was a significant predictor of a poor result after UKA. Age was not found to be a predictor of good outcomes in our study. Zuiderbaan et al.21) reported that age less than 65 years was a good predictor of improvement in the pain scale for the WOMAC score. Gender was not found to be a predictor of good outcomes in our study. Thompson et al.25) reported that female gender was associated with poorer outcomes following UKA. In fact, female patients and younger patients were found to have inferior functional outcomes following UKA in a meta-analysis conducted by van der List et al.29) Another controversial factor that is often debated is BMI. Our study did not find BMI to be a significant predictor of good outcomes following UKA. While the original set of classic indications for UKA exclude obese patients, there are emerging studies that show good outcomes even in this group of patients.2930) Zengerink et al.30) found that there was no significant difference in survival, patient reported outcome measures, or radiographic results following UKA between the obese and non-obese patients in their study.
The strengths of our study include that we used registry data, which were collected in a prospective fashion with highly detailed standardized information fields chosen to capture the outcomes of interest. This also ensured that all our patients undergoing medial UKA were enrolled and that the follow-up was completed at the appropriate follow-up time points. Another strength is our rigorous statistical model, which investigated a significant number of variables before obtaining the best predictive factors for UKA outcomes.
However, there were also some limitations. First, we used OKS and PCS as our outcome measures. Most of the literature on this topic utilized WOMAC scores and as such we could not conduct meaningful comparison. Second, while the study originated from an Asian nation, its results cannot be applied to all Asian countries due to the unique population demographics as well as the fact our cohort was predominantly female. Third, due to the lack of radiological data, we did neither include nor analyse radiological findings and outcomes. Fourth, our study evaluated midterm outcomes at 5 years as our registry is relatively new for UKA patients. Fifth, our results yielded odds ratios between 1.02 and 1.27. Despite significant, these were rather small and the confidence interval included 1.00 for two of the predictors. Therefore, the effect of these predictors in a clinical setting may be small. Sixth and most importantly, our definition of a good outcome was based on the achievement of the MCID and may not represent a clinically acceptable outcome. However, Hawker et al.12) have set a precedent for this definition of a good outcome. While using the MCID as the dependent variable in the regression has its merits, such a value for OKS and PCS has not yet been validated for an Asian population. However, this study does provide new insight into predictive factors of outcomes in medial UKA in Asians. In the future, the authors will utilize this model in a prospective fashion for validation in an Asian population.
In conclusion, patients with poorer OKS, PCS and KSKS, and better SF-36 MCS preoperatively tended to achieve good outcomes by the MCID criterion at 5 years following medial UKA.

 XML Download
XML Download