

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Legg-Calvé-Perthes disease (LCPD) is caused by an insidious circulation problem of the femoral head that usually results in collapse of the femoral head followed by secondary degenerative changes. LCPD usually results in pain and range of motion (ROM) limitations. In 1957, Salter first performed the innominate osteotomy to reduce congenital dislocation or subluxation of the hip. In 1962, based on his experimental investigations on a porcine model of LCPD, he began to apply the principle of innominate osteotomy to the subluxation associated with more severe forms of the disease.1) Salter innominate osteotomy (SIO) was used in special LCPD cases, for example, for lengthening or shortening extremities.234) However, its usage was limited because of technical difficulties as compared with the original SIO. SIO forms a horizontal line from the sciatic notch to the anterior inferior iliac spine at a right angle to the vertical axis of the ilium. Then, fixation of an inserted full-thickness triangular bone fragment is necessary. In 2003, we reported our modified SIO technique. Instead of performing an osteotomy from the sciatic notch to the anterior inferior iliac spine in one straight line, we made two plane osteotomy lines. The posterior half of the ilium from the sciatic notch was cut in the same manner as in SIO, but the anterior half was osteotomized using a reciprocal saw at 45° oblique to the coronal plane and 30° to 40° posteroinferior to the sagittal plane. It allows for tight and stable insertion of a triangular fragment without additional fixation.
In a previous study, we had evaluated the clinical and radiographic results of our modified SIO technique in 16 LCPD hips.5) The present study was undertaken to evaluate the long-term results of this modified SIO technique in LCPD patients followed until physeal closure.
METHODS
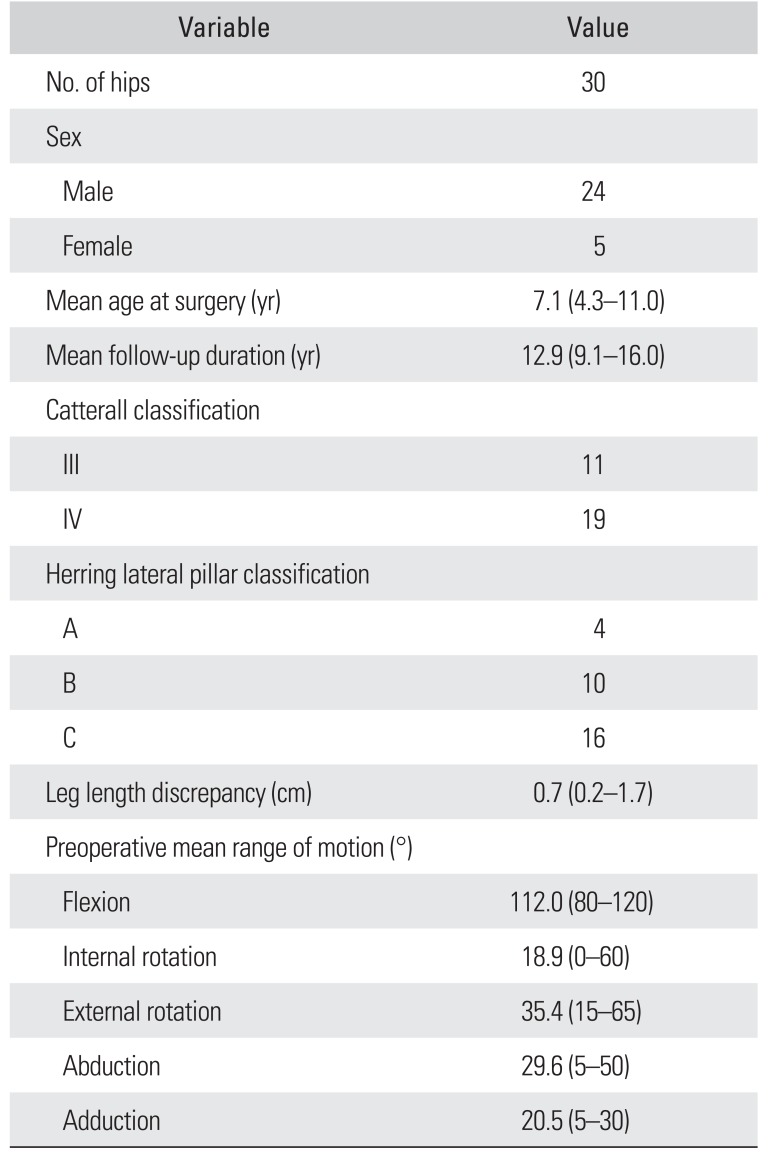
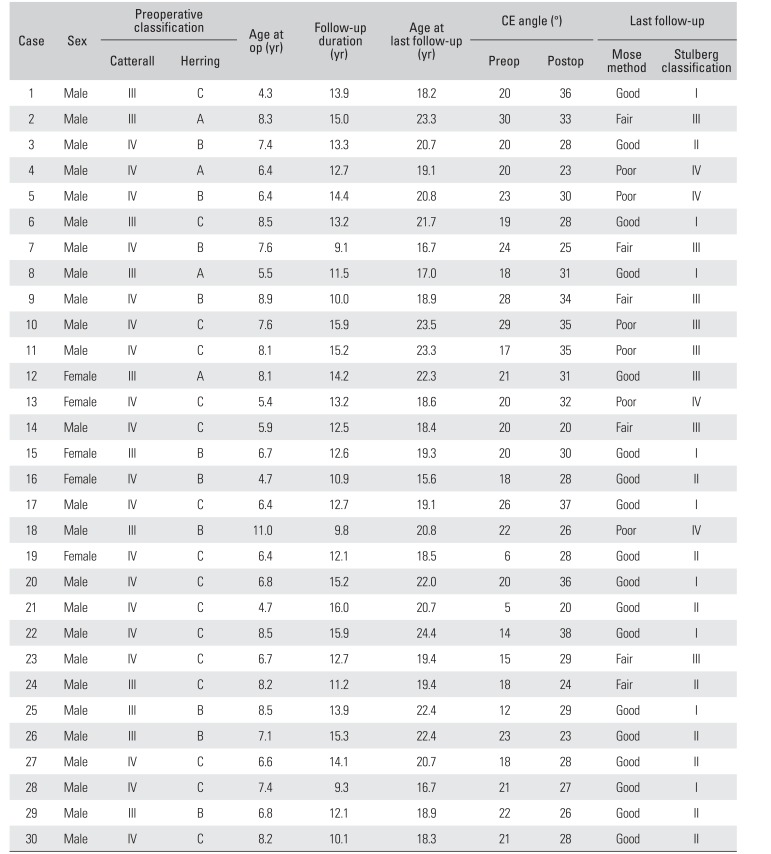
Between February 1998 and September 2001, we used the modified SIO in 33 hips of 32 patients of Catterall2) group III or IV.5) Three of the 32 patients were not able to be followed until skeletal maturation and thus were excluded from this study. Therefore, the study group consisted of 30 hips of 29 patients (24 males and five females). Their mean age at the time of surgery was 7.1 years (range, 4.3 to 11.0 years) and the mean follow-up was 12.9 years (range, 9.1 to 16.0 years). The indications for the modified SIO were involvement of more than half of the femoral head (Catterall groups III and IV) and loss of containment of the femoral head. A bioscrew was used to fixate the bone fragment after modified SIO in nine hips, but 21 hips received no additional fixation. Iliopsoas tenotomy was performed in 25 hips for flexion contractures of more than 30° and adductor tenotomy was performed in two hips with hip abduction of less than 30°. Catterall2) and Herring6) classifications were used to assess the extent of femoral head involvement in all hips. Eleven hips (36.7%) were classified as Catterall group III, and 19 (63.3%) as group IV. Four hips (13.3%) were classified as Herring group A, 10 (33.3%) as group B, and 16 (53.3%) as group C (Table 1).
Clinical assessment at the final follow-up was conducted using the Harris Hip Score (HHS)7) and Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) score.8) In addition, the ability to perform other hip positions common assumed among Asians, such as squatting and sitting on the floor, and the Buddhist position, were also evaluated. We also assessed results using the criteria suggested by Robinson et al.,9) according to which a result is considered good when the hip demonstrates a normal ROM and the patient is symptom-free, fair when hip movement (especially internal rotation) is slightly limited and the patient has no symptoms, or poor when hip movement is significantly limited and pain is experienced at rest or after physical activity. A limited ROM of the hip was defined as < 20° in abduction and internal rotation or < 100° in flexion and a side-to-side difference of ≥ 10° in abduction or ≥ 30° in flexion.10)
Preoperative and final radiographs were assessed by two orthopedic surgeons (SHL and HYY) using Wiberg's center-edge angle,11) the Mose method,12) and Stulberg classification.13) Osteoarthritic changes were evaluated using the Tonnis classification.14) Also, we analyze the relation of Stulberg classification with age and Herring's lateral pillar grade, which are established prognostic factors.
The independent t-test and chi-square test were used to determine the significances of differences between means and to analyze the influence of the prognostic factors, respectively. IBM SPSS ver. 19.0 (IBM Corp., Armonk, NY, USA) was used for all statistical analyses, and p-values of < 0.05 were considered statistically significant.
RESULTS
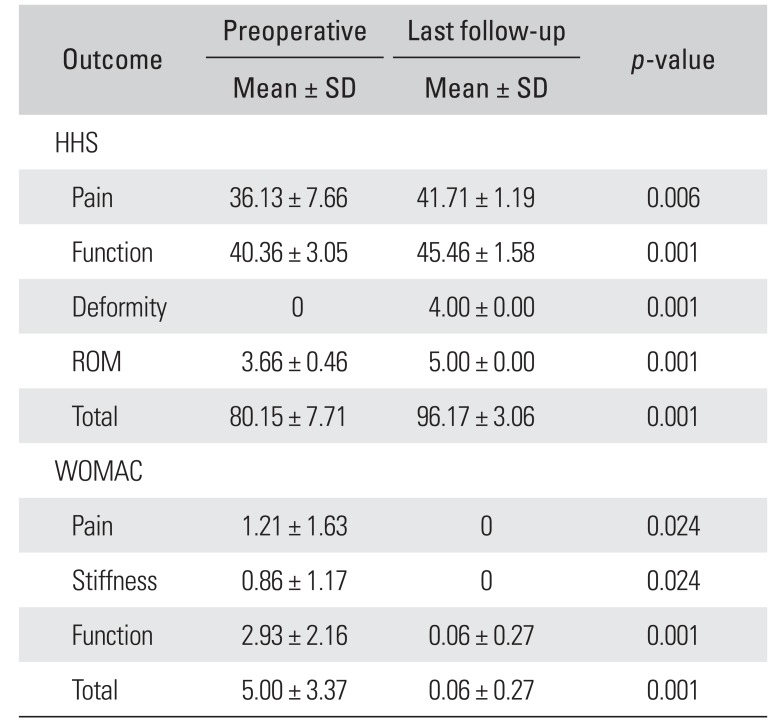
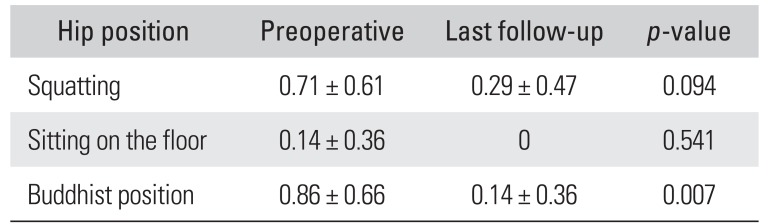
The mean HHS was 80.2 points (range, 70 to 92 points) prior to surgery and 96.2 points (range, 93 to 100 points) at the final follow-up (p = 0.001). The mean WOMAC score improved from 5 points (range, 1 to 11 points) preoperatively to 0.06 points (range, 0 to 1 points) at the final follow-up (p = 0.001) (Table 2). Improvement in the Buddhist position was also statistically significant at the final follow-up (p = 0.007) (Table 3). According to the criteria of Robinson et al.,9) 18 hips (60.0%) were good; seven (23.3%) were fair; and five (16.7%) were poor at the last follow-up. Twenty-four hips had decreased ROM compared to the preoperative value and six hips had restricted movement at the final follow-up. At the last follow-up, three hips were Tonnis classification grade 2; five hips were grade 1; and 22 hips were grade 0. Of the three hips with grade 2, two hips underwent Chiari osteotomy 12.1 and 8.8 years postoperatively, and the other hip underwent total hip arthroplasty 12.9 years postoperatively. With the exception of these two hips that underwent Chiari osteotomy, no other hip was painful, and patients with limited ROM did not experience any difficulty with the activities of daily living (Fig. 1).
The mean center-edge angle of the affected side increased from 19.7° (range, 5° to 30°) preoperatively to 29.6° (range, 19.6° to 38°) at the final follow-up. According to the Mose method, 18 hips (60.0%) were good; six (20.0%) were fair; and six (20.0%) were poor. According to the Stulberg method, nine hips (30.0%) were class I (good prognosis); nine hips (30.0%) were class II; eight hips (26.7%) were class III; and four hips (13.3%) were class IV (Table 4).
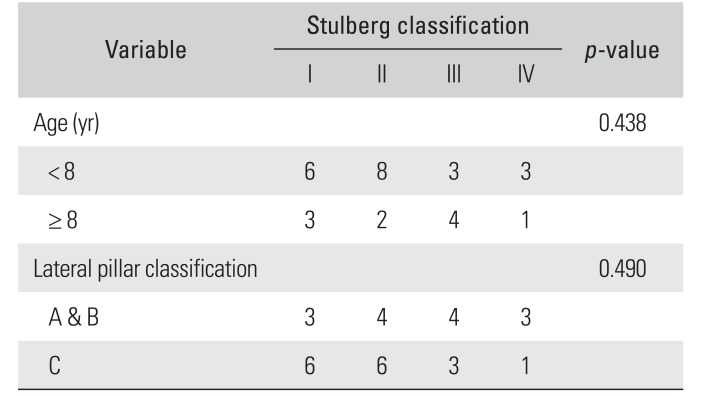
On the analysis of the influence of the established poor prognostic factors on Stulberg classification, which are age over 8 years and lateral pillar classification C, no statistically significant relationship was noted (Table 5).
DISCUSSION
It is difficult to determine the best treatment for LCPD diagnosed by clinical symptoms and abnormal radiological findings because the cause, pathology, and natural course have not yet been completely elucidated. Nonetheless, the general principle of treatment is “containment.” If a femoral head is well-contained in the cartilage mold, even in the case of collapse and deformation, it tends to be remodelled to a spherical shape, and when the femoral head finally reossifies, it becomes congruent with the acetabulum. 1516)
Olney and Asher17) reported that the treatment choice depends on the physician's preference, patient's choice, and level of activity. Of the surgical techniques designed to prevent deformity of the femoral head, the innominate osteotomy and femoral osteotomy have been most commonly used. Moreover, despite the lack of uniform clinical assessment for patients with LCPD treated by SIO,9151819) the reported incidence of physical impairment is low. Furthermore, several long-term follow-up studies have shown that patients with even marked deformities may have only mild symptoms for a long period.1213)
Our modified SIO5) differs from the original technique4) mainly in terms of the oblique osteotomy. The interposition of a triangular bone fragment facilitates achievement of required stability without internal fixation, producing the same limb lengthening effect as the Salter's osteotomy (about 1 cm). In SIO, the osteotomized bone fragment is fixed with a Steinmann pin, a hip spica cast is applied for 6 weeks, and weight-bearing is started 4 to 6 weeks after removal of the hip spica cast. On the other hand, our modified SIO requires no internal fixation or biodegradable screw fixation. However, a double splint should be applied postoperatively and intermittent active and assisted motion needs to be initiated the following day.
Salter4) reported one case of superficial wound infection and one case of osteonecrosis of the femoral head after osteotomies performed on 25 hips. Canale et al.18) reported two cases of pin tract infection and three cases of graft slippage after SIO performed on 120 patients. We have experienced no operative complications, but care should be taken to retain the subperiosteal plane throughout the modified SIO procedure because of the proximity of the sciatic nerve and the superior gluteal artery when periosteum of the inner surface of the ilium is stripped off to expose the sciatic notch.
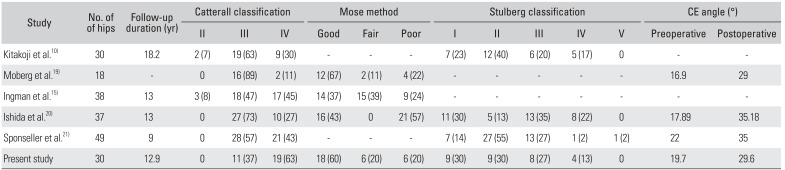
Several studies have reported on the results of SIO (Table 6). Salter16) reported 77% good, 17% fair, and 6% poor results according to the Mose method12) 50 months postoperatively. Ishida et al.20) reported clinical and radiographic results of 37 hips at skeletal maturity. Clinical results showed no correlation between sex, age, evolutionary stage and the Catterall2) and Mose12) classifications. Plain radiography at the final follow-up showed good results in 43.3% and poor results in 56.7%.
Kitakoji et al.10) reported that five of 30 hips with no preoperative restriction of motion were restricted after the Salter osteotomy. Moberg et al.19) reported that four hips in a femoral osteotomy group (16 patients) and four in an innominate osteotomy group (18 patients) had limited passive internal rotation. Ingman et al.15) compared 38 LCPD hips treated by innominate osteotomy with 33 hips, which were matched for age and severity and treated by recumbency in plaster hip spicas. Results were similar in the two groups although radiological results in the innominate osteotomy group were marginally worse. Sponseller et al.21) compared 49 innominate osteotomies with 42 femoral osteotomies and reported no difference in clinical results although the center-edge angles, neck-shaft angles, limb lengths, abduction ranges, and total ROM were closer to normal after the innominate osteotomy (Table 6).
In the present study, only five of 21 hips with a limited ROM preoperatively had a limited ROM postoperatively. In other words, unlike in previous reports,10151921) limited ROM was improved postoperatively in the majority of patients in our study. We attribute this to (1) iliopsoas tenotomy and adductor tenotomy that were performed in cases with flexion contracture or limitation of abduction and (2) passive movement exercises that were started shortly after surgery with the aim of increasing hip joint ROM.
Femoroacetabular impingement (FAI) after innominate osteotomy has been reported in some studies. Castaneda et al.22) reported the incidence as 12% (18 of 154 hips) among patients who had undergone Pemberton osteotomy and Salter osteotomy. FAI after innominate osteotomy was not common but the incidence was related to the angle of overcorrection in the study. Robb et al.23) reported 12% of acetabular retroversion after SIO without any sign of FAI. In our study, no patient complained of impingement symptoms at the last follow-up.
Several long-term follow-up studies have been conducted on the surgical treatment of LCPD. Nakashima et al.24) reported good 12-year results of trochanteric rotational osteotomy for late onset LCPD: 36% of the hips achieved a spherical, congruent status and 50%, a congruent status. Wenger and Pandya25) reported the results of two advanced surgical methods, combined SIO and triple pelvic osteotomy. They concluded that the triple innominate osteotomy might be a more attractive option because it allows relatively complete coverage of the femoral head (unlike SIO) while avoiding the risks of varus osteotomy of the femur.
Our study is limited by its retrospective design and the relatively small number of cases. In addition, most of the patients underwent the surgery before the indication of containment surgery was generally established and a consensus was made. However, it was a long-term follow-up study and the follow-up rate was high at 91% because most of the patients were male, and they had to undergo a check-up before being conscripted for obligatory military service.
In summary, our modified SIO technique requires less operative skill and can achieve stability without internal fixation due to the interposition of a bone fragment. Since the results of radiological and clinical evaluations of the modified SIO are comparable with those of SIO after physeal closure, we conclude that this simple and effective surgical modality maintains normal containment and sphericity of the femoral head.

 XML Download
XML Download