

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Among patients undergoing total knee arthroplasty, 60% experience severe postoperative knee pain and 30% experience moderate postoperative knee pain.1) Despite the postoperative pain, patients undergoing total knee arthroplasty are strongly recommended to initiate early ambulation and rehabilitation for satisfactory surgical outcomes. However, severe pain after total knee arthroplasty makes early ambulation and rehabilitation difficult, and can lead to knee stiffness, increase in hospital stay, and decrease in overall patient satisfaction.2) The severe postoperative pain eventually becomes the biggest reason for patients avoiding a contralateral total knee arthroplasty.3) Postoperative pain management modalities include the use of oral or intramuscular nonsteroidal anti-inflammatory drugs, opioid analgesics, intravenous or epidural patient-controlled analgesia, neuraxial analgesia (epidural analgesia), periarticular injection, and peripheral nerve blocks. Among these modalities, peripheral nerve blocks offer effective postoperative pain control and functional outcomes similar to those of continuous epidural analgesia and have a lower rate of complications related to epidural analgesia, such as generalized pruritus, dizziness, hypotension, and hematoma formation on the spine.4) In particular, femoral nerve block is often considered the gold standard for pain relief after total knee arthroplasty.45) However, femoral nerve block reduces quadriceps muscle strength and compromises early ambulation and rehabilitation. Moreover, it has been associated with higher risks of falls.6)
The adductor canal is located in the middle 1/3 of the thigh and runs from the apex of the femoral triangle proximally to the adductor hiatus distally. The adductor canal continuously encloses the saphenous nerve and the nerve to the vastus medialis. Placement of a catheter within the adductor canal can potentially spare the major motor branches of the femoral nerve while still providing effective postoperative pain control.78) However, only a few recent studies have compared the effect of femoral nerve block and adductor canal block on postoperative pain control after total knee arthroplasty. Furthermore, to our knowledge, no domestic study has compared the effect of femoral nerve block and adductor canal block on pain, quadriceps strength, and walking ability after primary total knee arthroplasty. The present retrospective study aimed to determine and compare the effect of continuous femoral nerve block and adductor canal block on (1) postoperative pain control; (2) postoperative quadriceps strength; and (3) walking ability after total knee arthroplasty.
METHODS
This retrospective study was approved by the Bumin Hospital Institutional Review Board (No. 201604-BM-007). We performed 30 femoral nerve blocks and 30 adductor canal blocks for postoperative pain control in patients who underwent primary total knee arthroplasty between December 2014 and February 2015.
We included patients over 55 years of age who had undergone primary total knee arthroplasty for osteoarthritis of more than Kellgren and Lawrence grade III and American Society of Anesthesiologists physical status classification of I to III. We excluded patients with a history of surgeries (contralateral knee surgery within 3 months and spine surgery within 6 months), allergy to any local anesthetics, history of chronic pain requiring treatment with long-acting opioids, inability to understand the numerical rating scale (NRS), and contraindications to peripheral nerve block (localized infections, sepsis, or preexisting lower extremity neurological abnormality).
All peripheral nerve blocks were performed before spinal anesthesia by the same anesthesiologist who had experience in ultrasound-guided peripheral nerve block. For the femoral nerve block, the femoral artery was palpated in the inguinal area. The tip of the needle was located 1–1.5 cm lateral to the femoral artery pulsation and 20 mL 0.75% ropivacaine was injected into the femoral nerve under ultrasound guidance (LOGIQ P6; GE Healthcare, Milwaukee, WI, USA). Then a 20-gauge catheter (Perfix; B. Braun Melsungen, Germany) was inserted for continuous nerve block. For the adductor canal block, the medial part of the thigh, the mid-portion between the superior anterior iliac spine and the patella, and the adductor canal were visualized under ultrasound guidance. In the axial view, we identified the femoral artery underneath the sartorius muscle and the saphenous nerve just lateral to the artery. With the tip of the needle placed just lateral to the artery and the saphenous nerve, 20 mL 0.75% ropivacaine was injected to expand to the adductor canal. Then a 20-gauge catheter was inserted for continuous nerve block. In both groups, the patients received repeated bolus injections of 10 mL 0.2% ropivacaine at intervals of 6 hours until the third day after surgery. Success of the block was verified by testing the response to a cold sensation determined by placing a cotton swab soaked with alcohol in the saphenous nerve distribution region. All patients had tricompartment cemented knee arthroplasty with posterior cruciate ligament (PCL)-substituting implants under tourniquet control. A standard medial parapatellar approach was used. All patients received intravenous patient-controlled analgesia (IV-PCA), which included fentanyl 600 µg (12 mL), ketorolac tromethamine 90 mg (3 mL), and nefopam hydrochloride 20 mg (20 mL) diluted in 150 mL saline: bolus, 5 mg; lock-out time, 20 minutes. Standard oral analgesics consisted of acetaminophen 325 mg, tramadol hydrochloride 37.5 mg, meloxicam 7.5 mg every 12 hours. On the first postoperative day, full weight bearing was allowed. But to prevent fall-down, patients ambulated with the assistance of a walker. And active and passive range of motion exercises with continuous passive motion and muscle strengthening were performed.
All patients' charts were reviewed retrospectively to obtain the outcome data. To evaluate postoperative pain control, the NRS scores at rest and at 45° flexion of the knee were recorded. To evaluate quadriceps strength, manual muscle testing (MMT) was performed. Walking ability was assessed using a validated ambulation test, the Timed Up and Go (TUG) test.9) The TUG test measures the time taken by a patient to stand up from a chair, walk a distance of 3 m, and return to the chair. All patients used a high walker with an arm support as an assisted walking aid to prevent falling during the test. The NRS scores and MMT results were accessed 4 times (6:00, 11:00, 16:00, and 21:00) a day on postoperative days 1, 2, 3, and one time on postoperative day 7. The TUG test result was measured once a day on postoperative days 1, 2, 3, and 7. To obtain highly objective results, one investigator assessed the MMT and TUG test results in all patients. We also evaluated the analgesic consumption and complications of peripheral nerve block in all of the patients.
Statistical analyses were performed using MedCalc (MedCalc ver. 15.2.2; MedCalc Inc., Mariakerke, Belgium). The Kolmogorov-Smirnov test was used to determine whether the measured and calculated parameters were distributed correctly. The independent samples t-test was used to determine the significance of intergroup differences in continuous variables. The chi-square test was used for association between 2 categorical variables. A p-value less than 0.05 was considered statistically significant.
RESULTS
The catheters were maintained in the exact location of the nerve block during the study period in 24 patients in the femoral nerve block group and 19 in the adductor canal block group. Almost all catheters were removed during continuous passive motion exercise or walking. The patients who had a catheter dropout during the study were excluded from collection of data for clinical outcomes.
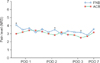
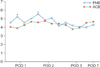
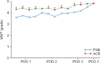
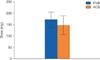
Patient demographics and clinical characteristics are shown in Table 1. The baseline values were similar between the 2 groups. The average time for femoral nerve block and adductor canal block was 9.8 minutes and 10.3 minutes, respectively, with no significant intergroup difference. Among the NRS scores obtained at rest, the one obtained in the first test on postoperative day 1, and those obtained in the third tests on postoperative days 2 and 3, showed significant intergroup differences. However, the groups generally showed no major differences (Fig. 1). Among the NRS scores obtained at 45° flexion of the knee, the one obtained in the second test on postoperative day 1, and the other obtained in the first test on postoperative day 2 also showed significant intergroup differences. However, the groups generally showed no major differences (Fig. 2). The adductor canal block group had significantly greater quadriceps strength than did the femoral nerve block group, as evidenced by the MMT results (Fig. 3). Walking ability measured using the TUG test showed no intergroup difference on postoperative day 1 (p = 0.181), but on postoperative days 2, 3, walking ability was significantly better in the adductor canal block group than in the femoral nerve block group (p = 0.03 and p = 0.019, respectively) (Fig. 4). None of the patients experienced any falls. Transient neuritis was observed in 2 patients in the femoral nerve block group and 3 in the adductor canal block group. No significant difference in the total amount of IVPCA and additional analgesic consumption (intramuscular tramadol hydrochloride injections) was observed between the 2 groups (p = 0.621 and p = 0.771, respectively) (Fig. 5).
DISCUSSION
The most important finding of this retrospective study is that the adductor canal block group had significantly greater quadriceps muscle strength than did the femoral nerve block group, without major differences in the NRS scores or analgesic consumption. Femoral nerve block is as effective as epidural anesthesia in pain relief, but without the associated side effects such as nausea, vomiting, and pruritus.45) However, femoral nerve block causes profound motor blockade that weakens quadriceps muscle strength. Jæger et al.7) showed that quadriceps strength reduces by 49% in healthy subjects undergoing femoral nerve block. Charous et al.6) reported an almost 80% reduction in quadriceps strength in human volunteers undergoing femoral nerve block even at a very low dose and volume. However, Jæger et al.7) reported that adductor canal block only reduced the quadriceps muscle strength by 8% compared with the baseline strength. Moreover, adductor canal block preserved the ability to ambulate better than did femoral nerve block.7) We judged that the influence of quadriceps weakness was reflected in the ambulation; therefore, we checked the TUG test results obtained on postoperative days 1, 2, 3, and 7. While we found no intergroup difference on postoperative day 1 (p = 0.181), we found that walking ability was significantly better in the adductor canal block group than in the femoral nerve block group on postoperative days 2 and 3 (p = 0.03 and p = 0.019, respectively). All subjects used a high walker with an arm support to minimize the risk of falling during the TUG test. This provided an opportunity to compensate for the quadriceps muscle weakness in the operated limb. If the TUG test was performed without an assisted walking aid, we think there might have been a significant intergroup difference in the TUG test results obtained on postoperative day 1.
None of the patients in the present study had falls. Because the sample size of this study was small and all patients were warned about the risk of falling, it was difficult to assess whether quadriceps muscle weakness did not increase the risk of falling. Several studies have shown that femoral nerve block was associated with a higher risk of falling,1011) which might be avoided with the use of adductor canal block. Therefore, more attention should be paid to avoid falls in patients undergoing femoral nerve block.
To evaluate postoperative pain control, the NRS scores at rest and 45° flexion of the knee were assessed. The NRS scores were somewhat lower in the adductor canal block group than in the femoral nerve block group, with some significant intergroup differences. However, we suggested that generally, no major differences appeared between the two groups at rest and during 45° flexion of the knee (Figs. 1 and 2). Total analgesic consumption was approximately 14.5% lesser in the adductor canal block group than in the femoral nerve block group, but with no intergroup difference. Therefore, we concluded that no significant intergroup difference existed in postoperative pain control. Our findings were similar to those of other comparative studies.71213) However, we did not have a control group because it is the standard protocol at our institution to provide a peripheral nerve block for postoperative pain management. Therefore, we are unsure how effective pain control with peripheral nerve block is compared to no peripheral nerve block in the control group. Future studies using appropriate control groups (no peripheral nerve block) are warranted to clarify this issue.
There is no consensus about the appropriate administration methods in peripheral nerve block. Generally, peripheral nerve block is administered in two ways: continuous technique and single-shot technique. In several studies, continuous peripheral nerve block showed better results than did the single-shot technique in optimal postoperative pain control after total knee arthroplasty.141516) Hunt et al.17) also reported that continuous peripheral nerve block yielded results superior to the single-shot technique in terms of pain control after the first 36 hours as well as opioid consumption. Shah et al.16) reported that continuous adductor canal block provided significantly superior results in terms of postoperative pain control than did single adductor canal block, without compromising walking ambulation and early functional recovery. Patients who underwent total knee arthroplasty at our institution are permitted ambulation and practice continuous passive motion exercises from postoperative day 1. Therefore, they complain of severe pain after rehabilitation. Controlling post-rehabilitation pain is as important as controlling operative pain; therefore, we preferred continuous peripheral nerve block.
The common complications of peripheral nerve block are catheter dropout, neuropathy, and infection. Among our patients who received femoral nerve block, 6 (20%) experienced catheter dropout, 2 (6.6%) developed neuropathy, and none developed any infection. Among those who received adductor canal block, 11 (36.6%) experienced catheter dropout, 3 (10%) developed neuropathy, and none developed any infection. Catheter dropout was defined as the visibility of the extraction or the persistence of pain after analgesic administration. Patient response to cold sensation was determined by placing an alcohol-soaked cotton swab on the distribution of the saphenous nerve on the upper medial part of the ankle and comparing it to the sensation on the contralateral side. The catheter dropout rate with adductor canal block was higher than that with femoral nerve block (p = 0.141). The catheter for adductor canal block is placed around the middle of the thigh, under a pneumatic tourniquet; this location results in a higher risk of catheter misplacement during surgery. The catheter must also be advanced through the sartorius muscle, and this might cause the catheter to be displaced during early rehabilitation and ambulation. Further studies may be needed to identify a technique for the successful maintenance of the adductor canal block catheter. In our study, 5 patients (8.3%) developed neuropathy. Nerve injury after peripheral nerve block is caused by direct injury, intraneural injection, hematoma formation, decreased blood flow, and infection. In this study, peripheral nerve block was performed under direct ultrasound guidance. Therefore, the neuropathies could be attributed to the decreased blood flow resulting from the use of a pneumatic tourniquet. Nevertheless, all patients recovered without additional treatment within an average of 16 days.
This study had some limitations. First, it was a retrospective, nonrandomized study. Differences in patient characteristics and surgical and nerve block techniques between the 2 groups may have affected the measured outcomes. To minimize the influence of confounding factors, we selected patients with similar baseline characteristics; moreover, the surgeries were performed by the same senior surgeon, and peripheral nerve blocks were performed by the same anesthesiologist by using standard protocols. Second, we performed MMT to compare the effect of femoral nerve block and adductor canal block on quadriceps muscle strength. MMT is a procedure for evaluating the function and strength of individual muscles and muscle groups based on the forces of gravity and manual resistance. MMT results depend on the investigator's subjective judgement, and they are difficult to precisely measure because of postoperative pain. Therefore, in our study, all MMT measurements were performed by the same experienced investigator to reduce any interobserver bias. Lastly, our study had a small sample size. This was because patients who had a catheter dropout were excluded from data collection for clinical outcomes. The statistical power negatively affected the likelihood that a nominally statistically significant finding actually reflected a true effect. To obtain precise results, studies on a larger sample size are necessary.
To conclude, no difference in pain control after total knee arthroplasty was observed between the adductor canal block and femoral nerve block groups. However, adductor canal block was superior to femoral nerve block in preserving quadriceps strength and walking ability. Compared to femoral nerve block, adductor canal block also provided better ambulation ability after total knee arthroplasty. However, adductor canal block was inferior to femoral nerve block in terms of the maintenance of nerve block.


 XML Download
XML Download