

 PDF
PDF ePub
ePub Citation
Citation Print
Print


The pathogenesis of rotator cuff tears is not clearly understood and controversial. Several studies proposed the extrinsic and intrinsic factors that contribute to rotator cuff tears. Neer12) described impingement of an acromion bone spur and the coracoacromial ligament on the rotator cuff tendon can lead to a tear. According to Codman,3) degenerative changes of the tendon were responsible for development of a tear. Regarding the extrinsic factors, Bigliani et al.4) made a classification of the acromion shape seen on a lateral radiograph into 3 types. There was a higher prevalence of rotator cuff tears with a hooked type acromion than with a flat or a curved type acromion.
Nyffeler et al.5) assessed the morphology of the acromion and compared the lateral extension of the acromion using the acromion index (AI) between the patients with a rotator cuff tear and those with an intact rotator cuff. The difference in AI between the groups was statistically significant (p<0.0001). Miyazaki et al.6) also compared the AI in Brazilian and Japanese populations considering a lateral tilt of the acromion as a possible cause of rotator cuff tears. The AI was significantly higher in the rotator cuff tear group in the Brazilian population suggesting the AI as a reliable predictor of a rotator cuff tear (p=0.01), whereas the AI was not significantly different between groups in the Japanese population. The paper states that there might be racial differences in the AI, and this should be examined in other Asian countries. Their paper stimulated our interest and we attempted to examine whether we could reproduce their results.
The purpose of this study was to assess the AI in a Korean population to determine whether any particular changes in the acromial structure are significantly associated with the presence of rotator cuff tears. Our hypothesis was that in the Korean population, morphologic differences in the acromion are associated with the etiology of rotator cuff tears.
METHODS
Patient Selection and Demographics
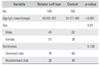
From January to December of 2013, 200 shoulders were retrospectively reviewed for this study and divided into 2 groups. One group included full thickness rotator cuff tear patients diagnosed by magnetic resonance imaging and intraoperative arthroscopic findings. The other group (control group) included patients with an intact rotator cuff tendon identified on magnetic resonance imaging and other shoulder diseases, such as frozen shoulder, instability, and calcific tendinitis. Exclusion criteria were partial thickness rotator cuff tears diagnosed on magnetic resonance imaging, previous surgery, fractures around the shoulder joint, arthritis, isolated subscapularis tears, osteonecrosis, and infection. The studied population was all Korean and exclusively Asian. There were 100 adults (mean age, 63 years; range, 42 to 87 years) in the rotator cuff tear group and 100 adults (mean age, 51 years; range, 17 to 84 years) in the intact rotator cuff group (control group). The rotator cuff tear group was composed of 57 men and 43 women and the control group consisted of 62 men and 38 women (Table 1). According to the classification of the cuff tear size suggested by DeOrio and Cofield7) the rotator cuff tears were categorized into small (< 1 cm) in 9 patients, medium (≥ 1 and < 3 cm) in 57 patients, large (≥ 3 and < 5 cm) in 23 patients, and massive (> 5 cm) in 11 patients for subgroup analysis. This study was approved by the Institutional Review Board of Samsung Medical Center (No. 2015-02-088).
Radiologic Assessment and Definition of AI
Two independent orthopedic surgeons with an 1-year experience in shoulder fellowship in our hospital assessed all radiographs and they were blinded to the diagnosis. Standard plain radiographs with a true anteroposterior (AP) view were obtained from all patients and assessed on picture archiving and communication system (Centricity Enterprise Web V3.0; GE Medical Systems, Milwaukee, WI, USA).
The true AP radiographs taken with the arm in neutral or internal rotation were used to assess the acromion as described in the study by Nyffeler et al.5) The observer drew three parallel lines on the AP radiograph and measured the distances between those lines. The first line connected the upper and lower tips of the glenoid rim. The second line was drawn on the lateral margin of the acromion parallel to the first line. The third line was drawn tangential to the most lateral part of the humerus head around the greater tuberosity. The AI was defined as the ratio of the distance from the glenoid to the lateral margin of the acromion (GA) divided by the distance from the glenoid rim to the lateral aspect of the humeral head (GH) (Fig. 1). A higher AI indicates a larger lateral extension of the acromion.
Statistical Analysis
Student t-tests were used to analyze the data and statistical significance was defined as a p<0.05. For subgroup analysis, Spearman correlation coefficient was calculated to test the association between the AI and tear size. Receiver operating characteristics (ROC) analysis and Youden8)'s index methodwere used to determine the cut-off value of AI for rotator cuff tears. To evaluate the inter-rater reliability of the data, the intraclass correlation coefficients (ICCs) of the different parameters were calculated. We considered an ICC of 0.8 or higher represents good or excellent reliability. Statistical analysis was performed with the IBM SPSS ver. 22.0 (IBM Co., Armonk, NY, USA) and SAS ver. 9.3 (SAS Ins., Cary, NC, USA).
RESULTS
Demographic data of the 200 patients are summarized in Table 1. The mean age of the patients was higher in the rotator cuff tear group than in the control group. In our opinion, the characteristics of degenerative disease appeared to have an impact on the difference. Sex and involvement of the dominant side were not significantly different between two groups. The ICC for AI was 0.82 showing good or excellent reliability. The mean AI was 0.68 in the rotator cuff tear group and 0.63 in the control group, showing a statistically significant intergroup difference (p<0.001) (Fig. 2). The mean AI was 0.68 in males and 0.69 in females, showing no statistically significant difference (p=0.236). Multivariate analysis was also performed to adjust for differences in age and sex distribution between groups, and no statistically significant difference was noted (p<0.001).
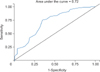
Subgroup analysis of the AI was done among the 4 subgroups that had different tear sizes. Spearman correlation coefficient was 0.03 and showed no statistically difference in the AI among the groups (p=0.74). The ROC analysis was performed to elucidate the optimal cutoff value of the AI for rotator cuff tears: the cut-off value was determined as 0.66 and the area under the ROC curve (AUC), sensitivity, and specificity were 0.72, 0.75, and 0.65, respectively (Fig. 3). According to the results, patients with an AI of 0.66 and above have a greater chance to have a rotator cuff tear and the accuracy of the test is fair (AUC, 0.72).
DISCUSSION
This study compared the AI in a Korean population and the results support those found by Nyffeler et al.5) in 2006. The difference in mean AI between the rotator cuff tear group and the intact rotator cuff group was statistically significant (0.68, p<0.001). Thus, the AI can be considered as a predictive factor for a rotator cuff tear. In the literature, many authors 59101112) also suggested the AI can be a possible cause of rotator cuff tears, but the relationship between the acromion morphology and rotator cuff tears is still controversial. In contrast, some authors demonstrated there was no significant association between the lateral coverage of the humeral head and the rotator cuff tear.13) In particular, Miyazaki et al.6) reported contrasting results obtained from two different races: the AI was a possible cause of rotator cuff tears only in a Brazilian population, not in a Japanese population. However, Moor et al.10) and Balke et al.14) recently described that distinct scapular morphologies including the AI accurately predicted the degenerative rotator cuff tear as radiologic parameters. Ames et al.15) reported there was an association between the AI and the outcomes of arthroscopic rotator cuff repairs in 120 shoulders. In the study, the authors demonstrated that the patients with a larger AI (> 0.682) had a greater chance to have a tear involving two or more rotator cuff tendons (p=0.017) and required more anchors for repair (p=0.007). Kim et al.9) also suggested the AI can be a predictor for progression to large-to-massive rotator cuff tears. Specifically, the highest differences in the AI were noted between the partial-thickness articular-side tears and large-to-massive rotator cuff tears (p<0.01). Fujisawa et al.16) reported results of three-dimensional analysis of the acromion shape. Rates of bony projection at the anterior (> 2 mm) and lateral (> 3 mm) edges of the acromion were significantly greater in patients with rotator cuff tears than those without (p<0.01). Acromial shape was not correlated with tear size (p=0.73). These findings are consistent with those in our study: the AI showed no statistically significant difference among the groups subdivided according to tear size (p=0.74).
There are several factors correlated with rotator cuff tears. Extrinsic factors refer to anatomic variables that compress the rotator cuff mechanically in impingement or under direct pressure from soft tissues.17) These include acromial spurs and morphological characteristics causing subacromial impingement18) or internal impingement.19) Intrinsic factors are related with degenerative changes within the tendon affected by vascularity or aging.20) However, the effects of these factors on the pathogenesis of rotator cuff tears remain unclear and the severity of symptoms is not proportionate to the size of a tear. According to recent studies, extrinsic factors including the AI can be powerful predictors for progression of rotator cuff tears.
The strengths of our study include that we evaluated a relatively large number of patients and confirmed the inter-rater reliability for the AI assessment, supporting the findings of Nyffeler et al.5) In addition, although the present study showed no relationship between the size of rotator cuff tears and the AI in the subgroup analysis, we elucidated the cut-off value of AI for rotator cuff tears in the Korean population.
There are several limitations in our study. First, it was a retrospective study, and the sample size was not sufficient to generalize the results to the entire population. Another limitation is mismatched demographic data. We excluded partial rotator cuff tear patients and included patients with instability and frozen shoulders. Accordingly, it was difficult to obtain substantial homogeneity in terms of age and gender due to the characteristics of shoulder disease. Third, technical errors could have been made while taking gleno-humeral (Grashey view) AP views to assess the AI. Finally, the glenoid and acromion shape can be affected during the natural progression of shoulder disease especially in rotator cuff tears. Although, the present study could not determine the relation between all the scapular anatomical characteristics and rotator cuff disease, we confirmed the AI is a possible cause of rotator cuff tears among various etiologies of rotator cuff disease. Further studies are required to confirm the pathogenesis of degenerative rotator cuff tears with other morphologic parameters.
In conclusion, contrary to a previous study suggesting the presence of racial difference with regard to the relationship between the AI and rotator cuff tears, our study showed that the AI was an effective predictive factor for rotator cuff tears in a Korean population.


 XML Download
XML Download