

 PDF
PDF ePub
ePub Citation
Citation Print
Print


One of the important functions of the intervertebral disc (IVD) is shock absorption with the vertebral endplate that enables spine to flex, extend and twist.1) Degeneration of the IVD is a physiological change associated with aging rather than disease, and it has a close relationship with the endplate. The vertebral endplates are typically less than 1 mm thick, and while this varies considerably across the width of any single disc, they tend to be thinnest in the central region adjacent to the nucleus.123) Moore1) reported that the Schmorl's node is an endplate defect caused by damage such as trauma. Vernon-Roberts4) argued that degenerative changes in the disc are more frequent in persons who have Schmorl's nodes and thus the endplate fracture is related to degenerative changes of the IVD. Some authors reported that pathological signal changes of the IVD on magnetic resonance imaging (MRI) can be observed after spine trauma, whereas others reported spine trauma has no relationship with pathological signal changes of the IVD.56)
The claim that endplate fractures are closely related to degenerative changes of the IVD is not novel. Kirkaldy-Willis et al.7) insisted that the spine becomes stabilized due to the limited movement with the progression of degeneration, whereas Stokes and Iatridis8) insisted that immobilization of the spine is related with degeneration of the IVD. Likewise, the relationship between spine immobilization and degeneration of the IVD is still controversial. To date, there have been many studies conducted on the effect of only endplate fractures or only immobilization on degeneration of the IVD. In contrast, this study evaluates degeneration of normal discs, immobilized discs, and immobilized discs with endplate fractures among patients who underwent posterior instrumentation without fusion for unstable burst fractures and instrumentation removal after fracture site healing. The aim of this study was to determine the relationship between degeneration of the IVD and spine immobilization under the hypothesis that immobilization accelerates degenerative changes.
METHODS
Patient Selection
We enrolled 57 patients who had been treated between September 1, 2003 and August 31, 2012 and met our inclusion and exclusion criteria (Table 1). All patients with an unstable burst fracture (Thoracolumbar Injury Classification and Severity Score [TLICS] > 5) which was not secondary to osteoporosis or pathological were managed by posterior instrumentation. This study was approved by the Institutional Review Board of Daegu Catholic University Medical Center (No. CR-14-055).
Treatment
The surgery was performed 2.4 days (range, 0 to 5 days) after injury using only the posterior approach. After insertion of a pedicle screw-rod system into the vertebra above and below the fractured vertebra via a paramedian approach between the multifidus and longissimus muscle, fixation was achieved by connecting rods while producing distraction. The insertion trajectory of the pedicle screw was from the lateral side of the facet joint to the vertebral body, striving for least violation of the adjacent facet joint. No laminotomies or laminectomies were performed. The fracture site was reduced by ligamentotaxis. No procedures to gain fusion were carried out, and there was no attempt at bone grafting of the vertebral body through the pedicle. If the pedicle of the affected vertebrae was appropriate for pedicle screw insertion, we performed short-segment pedicle fixation involving 2 levels above and 1 level below the affected vertebra. The patients were permitted to ambulate 2 or 3 days postoperatively using an external support such as thoraco-lumbo-sacral orthosis or lumbo-sacral orthosis. Implant removal was carried out between 8 and 14 months after the primary procedure with removal of other extremity implants.
Radiological Evaluation
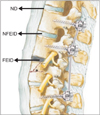
All patients were evaluated using plain radiographs, computed tomography (CT) scans, and MRI at the time of injury. Endplate fractures were diagnosed by presence of a displaced fracture line through the endplate on CT and MRI (Fig. 1). Based on MRI findings, we named the IVD that has an endplate fracture after immobilization using pedicle screws as fractured endplate and immobilized disc (FEID), the IVD that has no endplate fracture after immobilization using pedicle screws as nonfractured endplate and immobilized disc (NFEID), and the IVD that has no endplate fracture and no immobilization instrumentation as normal disc (ND) (Fig. 2). MRI was also performed 2 years after implant removal.
The degree of IVD degeneration was assessed using the Pfirrmann classification system9) (Table 2). The two MRI scans obtained at the time of injury and at 2 years after implant removal were reviewed by an orthopedic spine surgeon who was neither related to this study and nor participated in the surgery. If the difference in the extent of degeneration of the IVD on MRI between at the time of injury and at 2 years after instrument removal was over grade 2, degenerative changes were considered to have progressed (Fig. 3).
RESULTS
Epidemiologic Results
Among 57 patients, 40 were men and 17 were women. Their mean age at the time of injury was 39 ± 10.1 years (range, 16 to 53 years). Fractured levels were T12 in 10 (17.5%), L1 in 10 (17.5%), L2 in 19 (33.3%), and L3 in 18 (31.6%). More detailed disc distribution is shown in Table 3. The mean follow-up period (from the first MRI to the last MRI) was 28 months (range, 24 to 32 months).
Radiological Results
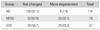
Among 259 IVDs of 57 patients, FEIDs were present in 67 levels, NFEIDs in 78 levels, and NDs in 114 levels. According to the Pfirrmann classification, 9 levels of the NDs (7.9%), 25 levels of the NFEIDs (32.1%), and 29 levels of the FEIDs (43.3%) were more degenerated at 2 years after implant removal. The NFEIDs and FEIDs were more degenerated than the NDs statistically significantly (p < 0.001). The FEIDs were more degenerated than the NFEIDs statistically significantly (p < 0.001). The highest percentage of degeneration was identified in the FEIDs followed by the NFEIDs and then NDs (Table 4).
DISCUSSION
A network of microscopic blood vessels penetrates the endplates during development of the growing spine, principally to provide nutrition for the disc, before disappearing around the time of skeletal maturity.110) Apart from a sparse vascular supply in the outer lamellae of the annulus, mature discs are almost totally reliant on diffusion of essential solutes across the endplates for nutrition and metabolic exchanges.111) An endplate fracture may induce pathological signal changes of the IVD on MRI, and inflammatory reaction accelerates degenerative changes of the IVD.561213) As mentioned above, there are many studies demonstrating the important role of the endplate in the IVD metabolism.17811)
Narrowing of the disc space has also been commonly observed after fractures of the thoracolumbar spine and associated with progressive kyphosis and pain in patients treated conservatively or with recurrent kyphosis after posterior reduction and fixation.141516171819) It is unclear whether this narrowing is a result of biochemical changes, as seen in degenerative disc disease, or narrowing represents an adaptation to changes in the morphology of the disc space as a result of the bony endplate fracture.20)
Some studies argued that radiological and histological disc degeneration can occur after 30s without trauma history and subjective symptoms.2122) In contrast, Oner et al.20) suggested that radiological signal changes after trauma means morphological changes rather than degenerative changes, and it is not degenerative disc space narrowing but a morphological change that occurs when the disc material leaks into the fractured site of an endplate of the vertebral body. This disc material can cause therapeutic failure or a secondary kyphotic change, but an endplate fracture alone is not enough for explaining IVD degeneration. Variable IVD injury patterns and therapeutic patterns are important for long-term stability of the spine,23) but not much else is known about adjacent disc degeneration and healing process.20)
There are many studies on the relationship of spinal cyclic loading and disc degeneration.24) Stokes and Iatridis8) noted that the mechanical condition of the IVD has a “safe window” and overloading of the IVD due to disc injury or delayed repair can cause problems. Immobilization may disrupt hemostasis of the IVD and accelerate degeneration of the IVD. As such, many studies insist that human spine degeneration can occur in immobilization or hypermobility of the spine.825) Therefore, controlled compression on the disc is essential to maintain healthy composition, structure, and mechanical properties of the spine.8)
Roaf observed that the discs are always stronger than the endplate under compression so that compression forces create a fracture of the endplate before causing damage to the IVD.26) According to Modic and Ross,27) endplate fractures do not violate the disc to cause its degeneration, but pedicle screw fixation can reduce cyclic loading to cause disc degeneration.
In this study we compared the MRI scans taken at the time of injury and 2 years after implant removal to evaluate the pedicle screw rigidity, fracture configuration, fracture reduction, underlying anatomy of the spine, stability of the fractured region by sagittal/coronal alignment and other variables according to degenerative changes of each disc.
One of the limitations of our study is the lack of evaluation on adjacent disc degeneration after instrumentation. According to various studies that address adjacent disc degeneration, degenerative changes do not appear to have correlation with clinical symptoms252829) and are observed at least several years and a decade afterward. However, our study dealt with short-term changes at around 4 years after immobilization. Therefore, further studies should be conducted on the relationship between clinical symptoms and degenerative changes in a longer follow-up. Demonstration of radiographic changes alone without clinical correlation is of little value. However, in the current study, we thought there was no need to assess clinical symptoms because the FEIDs, NFEIDs, and NDs were included in the analysis. It would be possible to determine the correlation between the extent of degeneration and the clinical symptom of each patient after long-term follow-up. Third, the possible difference in the degenerative change of the IVD between the thoracolumbar spine and that of the lumbar was not considered.
In conclusion, this study reaffirms that both endplate fracture and spine immobilization using transpedicular screw fixation without fusion play an important role in disc degeneration. The incidence of disc degeneration was highest in the fractured endplate and immobilization group followed by the immobilized and no fracture group. The group with normal appearing discs without immobilization showed the lowest incidence of disc. The differences among groups were statistically significant. Therefore, we think that spine immobilization with transpedicular screws has a significant influence on disc degeneration, and endplate fractures accelerate the degeneration process. Moreover, it appears that endplate fractures combined with spine immobilization without fusion have a greater impact on the degenerative process of IVD than endplate fractures alone.





 XML Download
XML Download