

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Hemiarthroplasty is now the treatment of choice for displaced fractures of the femoral neck in elderly patients.12) Hemiarthroplasty can be performed in two different ways: fixation with bone cement or press-fit without cement.
Early rehabilitation can be achieved with less pain after cement fixation by providing an immediate strong interlock between the prosthesis and the periprosthetic bone tissue.3) Cement fixation can decrease postoperative complications related to late mobilization, such as pneumonia or urinary tract infection (UTI), compared to cementless fixation.4) However, cementless fixation is associated with a shorter operation time and less intraoperative blood loss.5)
Until recently, five systematic reviews and meta-analyses comparing cemented hemiarthroplasty and cementless hemiarthroplasty have been published.678910) Most studies have evaluated mortality, postoperative pain, function, and general medical complication rates. However, no previously published meta-analysis has focused on infection-related complications.
The purpose of the current study was to assess the risk of postoperative complications related to infection after hemiarthroplasty in elderly patients. Therefore, we reviewed all up-to-date randomized clinical trials that reported on the followings: (1) postoperative deep infection; (2) postoperative superficial infection; (3) pulmonary infection; and (4) UTI.
METHODS
Search Methods for Identifying Studies
Two reviewers (BHY, JGS) independently searched PubMed, EMBASE, and Cochrane Library databases for eligible trials from September 3, 2016. The following search terms were used in the PubMed database: (hip [Medical Subject Heading term, MeSH] OR hip [all fields] OR hip joint [MeSH term]) AND (arthroplasty [MeSH term] OR arthroplasty [all fields]) AND (bone cements [MeSH term] OR bone cement [all fields] OR cemented [all fields]) AND (cementless [all fields] OR uncemented [all fields]) AND English [language]. In the other databases, the following keywords were used: hip, replacement, arthroplasty, bone cement, and cementless or uncemented. The identified studies were then filtered to limit the search to publications from 1980 to 2016.
Bibliographies of the selected articles were also reviewed manually to identify any articles not found in the primary search. Two observers (BHY, JGS) reviewed the titles and abstracts of the identified articles. If both observers agreed that a study did not meet the eligibility criteria, it was excluded.
Inclusion criteria were (1) randomized controlled studies on cemented and cementless hemiarthroplasty in patients with a femoral neck fracture and more than 65 years of age; and (2) articles reporting at least one of the following main clinical outcomes: the rate of superficial wound infection, deep infection, or general perioperative complications related to infection.
Exclusion criteria were (1) articles that included revision cases; (2) articles that used national registry data; (3) articles that reported no infection in both cemented and cementless groups; (4) articles that grouped reports of outcomes without distinguishing cases with complications in detail; and (5) reviews and basic science articles.
Data Extraction
Data, including the year of publication, study design, number of hips treated with hemiarthroplasty, type of implant used, technique of cement use, status of antibiotic loading in bone cement, mean length of follow-up, number of hips lost to follow-up, and time when infection occurred, were extracted and entered into a spreadsheet.
Outcome Measurements
The primary outcome was the rate of deep infection in patients who underwent hemiarthroplasty. Secondary outcomes were postoperative complications recorded as follows: (1) superficial wound infection treated with antibiotics only without surgery; (2) pneumonia; and (3) UTI.
Quality Assessment
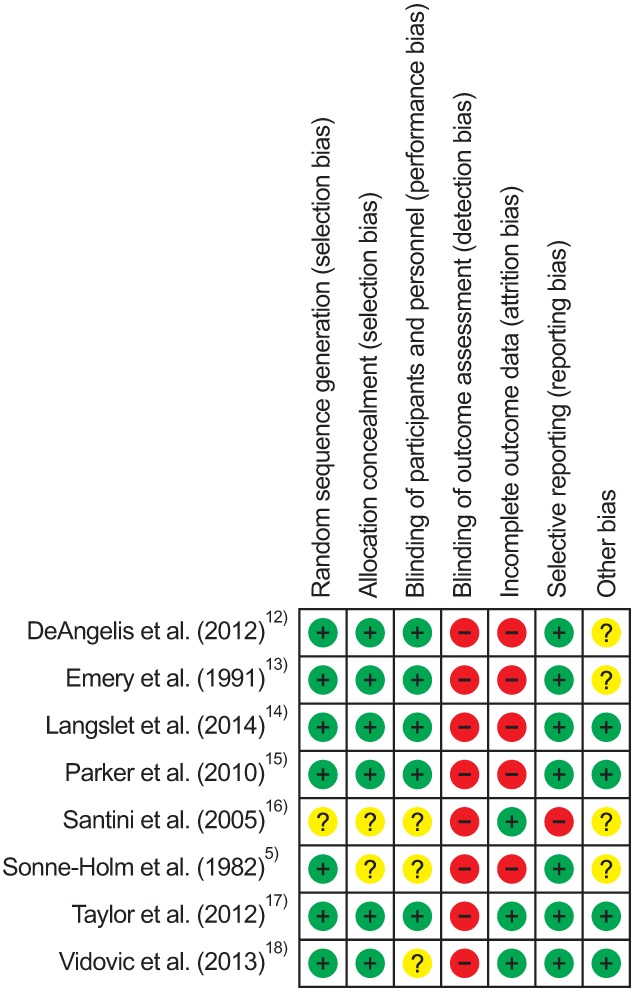
Reviewers (BHY, JGS) independently evaluated the methodological quality of the included trials using a specific tool for assessing the risk of bias recommended by the Cochrane Collaboration. This comprises a description and a judgment for each entry in a risk of bias table, in which each entry addresses a specific feature of the study. The judgment for each entry involves answering a question with one of the following responses: yes, indicating a low risk of bias; no, indicating a high risk of bias; and unclear, indicating either a lack of information or uncertainty over the potential for bias.11)
Data Synthesis and Analysis
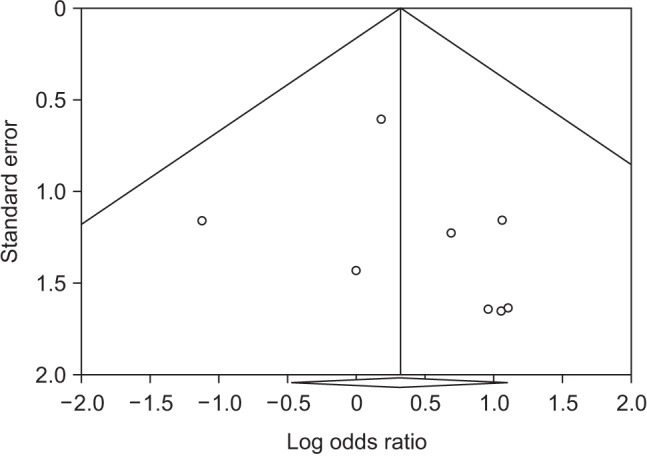
For each study, we calculated the relative risks with 95% confidence intervals by using crude 2 × 2 tables on the basis of intention to treat analysis, whenever possible, from the original publications.11) To test heterogeneity, we used Higgins I2 statistics. Significant heterogeneity was not observed in these studies (p = 0.957); therefore, we reported data from a fixed-effects model. We also performed meta-regression analysis to evaluate the association between the study's results and continuous variables. We assessed publication bias using Begg's funnel plot and Egger's test. If publication bias exists, the Begg's funnel plot is asymmetric or the Egger's test p-value is < 0.05. The meta-analysis was performed using Comprehensive Meta-analysis software ver. 3.3 (Biostat, Englewood, NJ, USA).
RESULTS
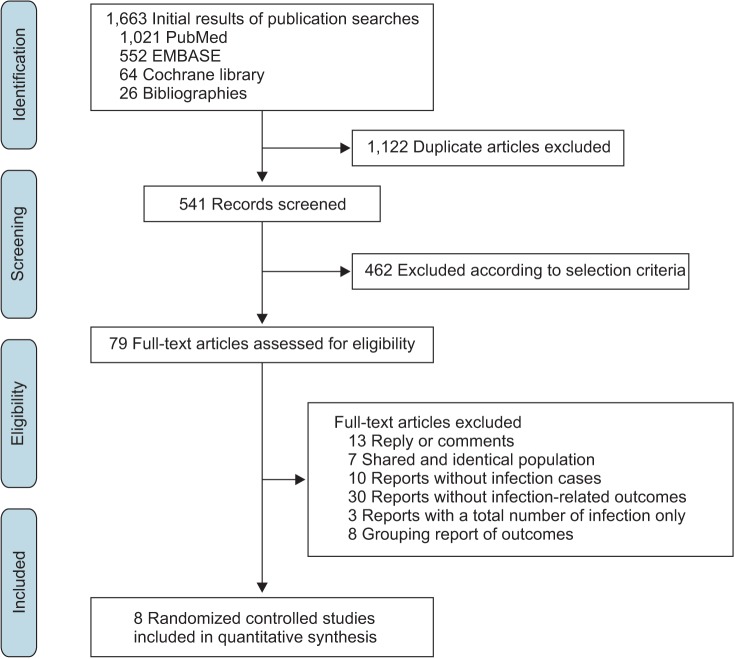
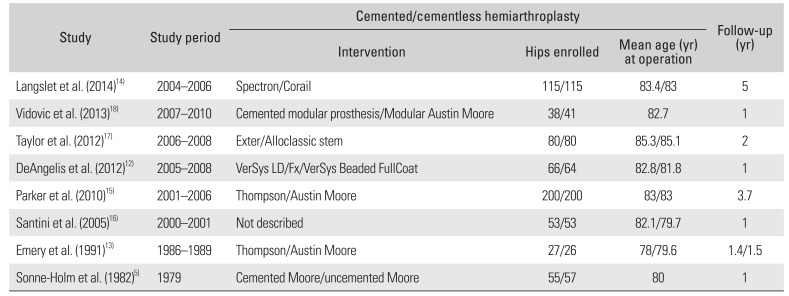
Based on the aforementioned search criteria, 8 randomized controlled trials were available for the final analysis. 512131415161718) The process from the initial publication searches to the final selection of clinical trials is displayed in a flowchart (Fig. 1). There were 1,204 hips included in the 8 studies: 608 hips in the cemented group and 596 in the cementless group. The study design, types of implants used, and included data extracted from each of the analyzed studies are summarized in Table 1.
The overall incidence of postoperative deep infection was 2.3% (14/608) in the cemented group and 1.2% (7/596) in the cementless group. The overall superficial wound infection incidence was 1.5% (9/608) in the cemented group and 1.7% (10/596) in the cementless group. The incidence of pneumonia and UTI were 3.6% (21/608) and 1.8% (11/608) in the cemented group, and 5.0% (30/596) and 2.2% (13/596) in the cementless group, respectively.
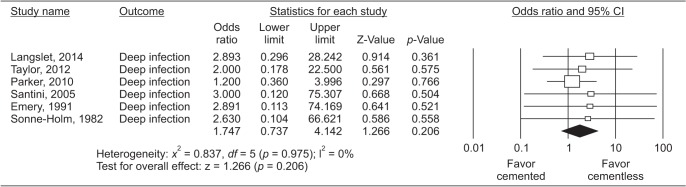
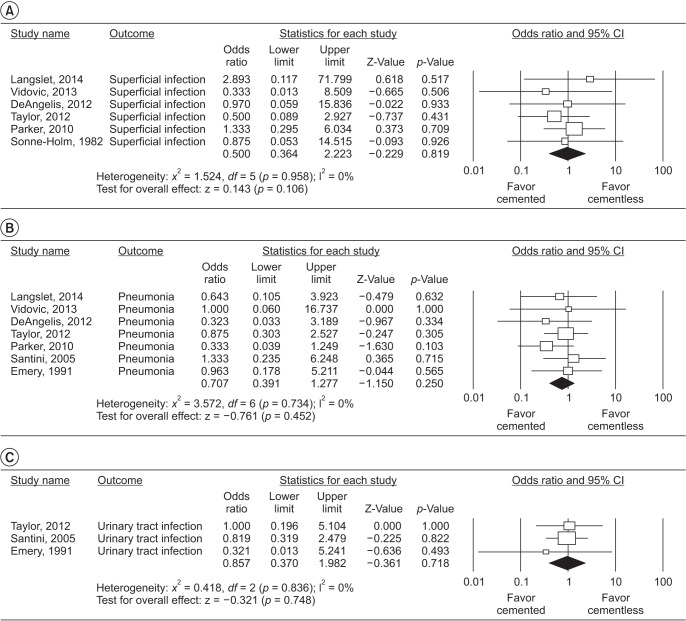
In the fixed-effects meta-analysis of all 8 trials, the use of cement was not associated with an increased risk of postoperative deep infection (relative risk, 1.74; 95% confidence interval, 0.74 to 4.14; I2 = 0%; p = 0.206) (Fig. 2). When the other infection-related outcomes were analyzed, no significant differences between cemented and cementless hemiarthroplasty were found (Fig. 3). We found no significant association between the odds ratio (OR) and the difference in operation time between two groups, year of publication, and duration of follow-up (Table 2).
DISCUSSION
Infection-related complications remain a potentially devastating complication, resulting in major morbidity for the patient, which adversely affects the outcome of arthroplasty. 19) Despite surgeons' best efforts, deep infection, in particular, can ultimately lead to a dysfunctional or disfiguring result.20)
Our meta-analysis showed no significant difference in the OR of postoperative deep infection between cemented and cementless hemiarthroplasty. The longer operating time for cemented hemiarthroplasty can be a risk factor for an increased incidence of infection.21) In the included studies of our analysis, the operation time was on average 11 minutes longer for cemented hemiarthroplasty than for cementless hemiarthroplasty.12131415161718) We additionally have performed meta-regression analysis on the OR and the difference in operation time between two groups, but no significant difference was found (Table 2).
It is interesting to compare this with our previous report in patients with primary total hip arthroplasty (THA).22) The previous review revealed that the use of cement in THA was associated with an increased risk of deep infection (OR, 1.53). In contrast, this analysis noted the risk of deep infection (OR, 1.74) in the cemented group showed no significant difference. The surgery time of hemiarthroplasty is usually much shorter than that of total hip arthroplasty.23) The surgery time of hemiarthroplasty takes only within 1 hour, it could not make a significant difference.24) Also, the cumulative sample size was not enough to demonstrate the significant difference although meta-analysis was performed. Similar postoperative deep infection rates after hemiarthroplasty between two groups were also observed from national registry studies (Table 3).252627)
Antibiotic-loaded bone cement and perioperative antibiotics have been shown to protect against infection in earlier studies.28) Additionally, perioperative transfusion of leukocyte-containing allogeneic blood components is an apparent risk factor for the development of postoperative bacterial infections.29) We attempted to perform subgroup analysis for cemented hemiarthroplasty, perioperative antibiotics, and blood transfusion. However, the use of perioperative antibiotic or antibiotic-loaded bone cement was described in only 4 studies,12141518) and blood transfusion was described in another 4 studies.5121516) Thus, we could not perform subgroup analysis in terms of antibiotics or blood transfusion.
Bone cement forms a solid bond between the stem and bone, providing favorable biomechanical advantages. This advantage can reduce the degree of early postoperative pain and lead to better mobility and early mobilization. Thus, we expected lower postoperative complication rates such as pneumonia by early ambulation or UTI via the early removal of an indwelling urinary catheter.4) There was no significant difference; however, the overall incidences of pneumonia and UTI were slightly lower in the cemented group than in the cementless group.
Cementless fixation is preferred in patients with a high risk of perioperative mortality.30) Serious intraoperative complications, including intraoperative death and cardiac arrest, were almost exclusively reported for the cemented procedures.25) In randomized studies, the suitability of each patient who received a cemented component was assessed by the anesthetist in charge, and patients whose risk of mortality was deemed unacceptable were excluded from the study.17)
The present study has some limitations. First, the cumulative sample size was not very large because most of the trials included relatively few hips. However, we additionally performed sample size calculation based on an OR (1.53) to estimate the required sample size: a total of 806 patients would be sufficient to detect difference with a power of 0.80 and a two-tailed alpha of less than 0.05. The number of subjects included in our study (1,204) was enough to detect difference. Second, potential sources of bias in these trials included a lack of blinding to the type of surgical treatment by the outcome assessors, an increased loss to follow-up, and postrandomization exclusion of study participants from analyses in several trials.
There is still debate about the choice between using cemented and cementless hemiarthroplasty for treating femoral neck fractures in elderly patients. In our meta-analysis, there were no significant differences in the postoperative complication rates between cemented and cementless hemiarthroplasty. Our meta-analysis suggests that when selecting a fixation method for hemiarthroplasty, infection-related postoperative complications are not a determinant factor to consider. Thus, the choice of implant for hemiarthroplasty can be made based on other factors such as the patient's comorbidities or the surgeon's preference.


 XML Download
XML Download