

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Restoration of lumbar lordosis is important for the maintenance of sagittal balance.123456789) Posterior spinal fusion is the most frequently performed procedure for degenerative lumbar spinal stenosis. Flexible deformities may be corrected with careful intraoperative positioning and instrumented fusion.10) Surgeons frequently use an OSI (Jackson; Orthopaedic Systems Inc., Union City, CA, USA) frame to maintain lumbar lordosis during posterior spinal fusion.
If correctional osteotomy is not performed, physiologic lumbar lordosis has to be gained by intraoperative prone positioning with a hip extension and posterior instrumentation technique. Therefore, optimal positioning before instrumentation is important in the restoration of lumbar lordosis.
Some literature analyzes lumbar lordosis during intraoperative prone positioning.111213141516) There is a study which reported that as the body mass index (BMI) increases, intraoperative lumbar lordosis also increases.17) Harimaya et al.18) reported that patients with preoperative hypolordosis had an enhanced lumbar lordosis after positioning alone compared with their preoperative upright radiographs but patient with substantial preoperative lordosis remained unchanged. However, there is no study that has analyzed the effects of types of spinal stenosis on intraoperative lumbar lordosis.
The purpose of this study was to evaluate change of lumbar lordosis from the upright position to intraoperative prone positioning on the Jackson table and to evaluate the effect of spondylolisthesis on lumbar lordosis on OSI frame.
METHODS
Sixty-seven patients who underwent posterior fusion due to spinal stenosis from May 2007 to February 2012, were included. In order to be included in the study, the patients had to meet the following criteria: (1) be over 50 years old at the time of surgery; (2) undergo an instrumented posterior spinal fusion on the lumbar spine for the treatment of spinal stenosis; (3) not have any anterior fusion; and (4) not have had a previous spinal fusion on the lumbar spine.
Thirteen males and 54 females meet these criteria. They had an average age of 67.86 ± 8.48 years (range, 50 to 85 years) at surgery. Patients, who had spondylolisthesis in the lateral radiograph of the lumbar spine with or without spondylolysis, were divided into spondylolisthesis group. Patients with simple stenosis (SS) were included in the SS group. Among all patients, 24 patients were diagnosed with simple spinal stenosis, 43 patients with spondylolisthesis (29 degenerative spondylolisthesis and 14 isthmic spondylolisthesis). The average BMI was 25.1 ± 3.3.
Operative Position
All patients were positioned in a standard manner on the OSI frame equipped with two chest pads and two pelvic pads. The chest pads were placed slightly distally to allow the axilla to remain free, and the pelvic pads were centered just distally to the anterosuperior iliac spine to allow the abdomen to also hang free. The knees and shins were placed on pillows on top of flat boards with the knees in slight flexion (Fig. 1).
Measurement of Lumbar Lordosis
Lumbar lordosis was measured from the upper end plate of L1 to the upper end plate of S1 on a preoperative upright position, intraoperative prone position and postoperative upright position after 12 months from the operation date when the fusion mass was gained. Using the Cobb method two spinal surgeons who were not part of the operative team performed the measurements.
To standardize lateral radiographs in an upright position, patients were told to stand up straight with their knees fully extended and their arms resting horizontally on a stabilizing bar at chest level. A lateral radiograph of the lumbar spine was checked in the prone position on the Jackson frame before performing a subperiosteal dissection of the lumbar spine to achieve a level-marking radiograph on all patients. Therefore, the measurement represented values for the intact paraspinal muscle, facet joints and all posterior ligaments.
Paired t-test and chi-square tests were used to statistically evaluate the difference between the two groups. In addition, the risk of increased lordosis on the OSI frame was analyzed using a binary logistic regression test controlling age, gender and BMI. The difference was considered statistically significant when the p-value was less than 0.05.
RESULTS
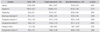
The preoperative average lordosis angle was 43.5° ± 14.9° and the intraoperative average lordosis angle on the Jackson frame after general anesthesia was 48.8° ± 13.2°. The average increase in the lordosis angle from the upright to prone position was 5.3° ± 10.6° and the postoperative average lordosis angle 12 months after the operation was 46.5° ± 16.1° (Table 1).
Among all patients, 24 patients were in the SS group, and 43 patients were in the spondylolisthesis group (29 degenerative spondylolisthesis and 14 isthmic spondylolisthesis).
The preoperative average lumbar lordosis angle was 38.15° ± 14.54° for the SS group, and 46.43° ± 14.45° for the spondylolisthesis group. The average preoperative lumbar lordosis of the spondylolisthesis group was significantly higher compared to the SS group (p = 0.028).
The intraoperative average lumbar lordosis angle of the SS group was 41.04° ± 11.57°, and that of spondylolisthesis group was 53.11° (± 12.12°). The average intraoperative lumbar lordosis of the spondylolisthesis group was significantly higher than in the SS group (p < 0.001).
The postoperative average lumbar lordosis angle of the SS group was 39.00° ± 15.95°. The average of the spondylolisthesis group was 50.65° ± 14.85°. The postoperative lumbar lordosis angle of the spondylolisthesis group was significantly higher than in the SS group (p = 0.004) (Table 1).
The average change of the lumbar lordosis angle on the Jackson frame from the upright position to the intraoperative prone position was 2.88 ± 9.88 in the SS group. The average change of the lumbar lordosis angle in the spondylolisthesis group was 6.67 ± 10.87 and was not significantly different from the SS group (p = 0.162).
However, the percentage of patients with increased lordosis on the OSI frame compared to preoperative lordosis was 50% in the SS group and 74.4% in the spondylolisthesis group. The ratio of patients with increased lordosis on the OSI frame was significantly higher in the spondylolisthesis group (p = 0.044). The ratio of gender and obesity was not significantly different between the two groups (Table 2). The risk of increased lordosis on the frame was significantly higher than in the spondylolisthesis group (odds ratio, 3.325; 95% confidence interval, 1.101 to 10.039; p = 0.033) (Table 3). The ratio of gender and obesity was not significantly different between the two groups (Table 2).
DISCUSSION
Preservation of lordosis during instrumented lumbar fusion is important in the maintenance of normal sagittal alignment. Wang et al.19) reported that correcting sagittal parameters while treating sagittal imbalance is important for attaining a better quality of life. Hip flexion was associated with a significant decrease in lordosis in patients and positioning in maximal hip extension optimizes lordosis preservation.14) Therefore, in patients with degenerative spondylolisthesis or isthmic spondylolisthesis, the removal of a proximal thigh pad will be needed if segmental hyperlordosis is present in the lateral radiograph during level checking.
Harimaya et al.18) reported that patients with preoperative hypolordosis who were positioned prone during reconstructive surgery had an enhanced lumbar lordosis via positioning alone compared with their preoperative upright radiographs. Conversely, those with substantial preoperative lordosis remained unchanged with intraoperative prone positioning. In this study, the average of preoperative lumbar lordosis was 38.15 in the SS group, and 46.43 in the spondylolisthesis group. The average increase on the Jackson frame in the SS group was 2.88, and 6.67 in the spondylolisthesis group. The SS group that had relatively smaller lordosis had a smaller increase in lumbar lordosis compared to the spondylolisthesis group.
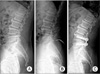
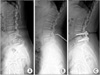
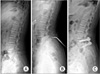
Lee et al.13) reported that intraoperative total lumbar lordosis was significantly decreased compared with the preoperative value and intraoperative position does not affect postoperative total lumbar lordosis and segmental lordosis in short-segment fusion. In our study, postoperative lumbar lordosis was significantly higher in the spondylolisthesis group. Due to an increase in segmental lordosis in the spondylolisthesis group at the fusion level in which instability exists, intraoperative lumbar lordosis also increases. In contrast, the fusion segment in the SS group was already stabilized as a result of degenerative change, so the increase was minimal after being in the prone position (Figs. 2,3,4). This may result in increased lumbar lordosis in the spondylolisthesis group rather than in the SS group.
Marsicano et al.20) reported that performing adolescent idiopathic scoliosis correction on the OSI frame tends to decrease thoracic kyphosis, increase thoracolumbar lordosis, and increase segmental instrumented lumbar lordosis, while it maintains total lumbar lordosis. In this study, the ratio of patients whose lumbar lordosis increased from the upright to prone positioning was higher in the spondylolisthesis group. This result may be attributed to segmental hyperlordosis in the spondylolisthesis group on the Jackson frame. Measurement of segmental lordosis in each group will be needed to further evaluate that cause.
There are some debates about the optimal operative frame for posterior lumbar fusion surgery. Peterson et al.16) reported that the "90–90" position on the Hastings frame was associated with a significant reduction in the total and segmental lordosis in the middle and lower lumbar spine and positioning prone on a Jackson table maintained standing lumbar lordosis and increased lumbosacral lordosis. However, there is a study that reposted that no significant difference was found in lumbar lordosis between the standing and chest roll positions. However, there was approximately a 50% reduction in lumbar lordosis when using the Hasting's, Andrew's, and four-poster frame compared to the standing and chest roll configuration.21)
Overall, lumbar lordosis is well maintained in patients undergoing short-segment instrumented fusion in the kneeling position. With compensatory lordosis being shifted proximally and the sacral tilt not returning to the preoperative status in L4–S1 fusions, caution should be exercised in using the kneeling position for longer instrumented lumbar fusions.22) However, most lumbar lordosis is present in the distal lumbar spine, and it is important to make normal segmental lordosis even in short segment fusion especially when performing surgery in the lower lumbar region. Most of our cases were performed on the lower lumbar region.
Vialle et al.23) reported that increased lumbar lordosis associated with L5–S1 spondylolisthesis is secondary to the high pelvic incidence and is an important factor causing high shear stresses at the L5–S1 pars interarticularis. In our study, lumbar lordosis in the spondylolisthesis group with spondylolysis was increased on the OSI frame due to increased segmental lordosis of L5–S1 with anterior rotation of the pelvis. This segmental instability owing to pars defect may contribute to increased lumbar lordosis on the OSI frame in the spondylolisthesis group with spondylolysis.
The weakness of this study is the selection bias of the spondylolisthesis group that has increased lumbar lordosis on the OSI frame, because most patients have preexisting segmental instability before surgery. Further study is needed for patients with degenerative spondylolisthesis or isthmic spondylolisthesis without segmental instability.
Intraoperative lumbar lordosis on the OSI frame with a prone position was larger in SS patients than in spondylolisthesis patients. Intraoperative lumbar lordosis on the OSI frame with a prone position also produced a larger postoperative lordosis angle after posterior spinal fusion surgery. Increase in lumbar lordosis on the OSI frame should be considered during posterior spinal fusion surgery, especially in spondylolisthesis patients.



 XML Download
XML Download