

 PDF
PDF ePub
ePub Citation
Citation Print
Print


A unicameral bone cyst, otherwise known as a simple bone cyst, is a common benign lesion that usually occurs in the long bone of a growing child. It is a fluid-filled cavity in the bone, lined by compressed fibrous tissue. More than 95% of these lesions involve the metaphysis of the long bone, especially the proximal humerus and the proximal femur.1) Involvement of other sites such as the diaphysis of long bones is uncommon. Usually, diaphyseal location of the lesion occurs because it moves from the metaphysis to the diaphysis during bone growth.2) In the case of the lesion of diaphyseal origin, recurrence at the same location is extremely rare.
Many theories have been proposed on the etiology of unicameral cysts since first described by Virchow in 1876; however, the exact etiology remains unknown. One theory is that the cysts result from a localized failure of ossification.3) Another theory suggests that the cysts arise from problems with circulation that are caused by a developmental anomaly in the veins of the affected bone.4) The role trauma plays in the development of these cysts is unknown.
The current study describes an interesting case of a patient who had recurrence of a unicameral bone cyst in the diaphysis of the femur after curettage and bone grafting. We propose a possible etiology of the lesion based on long-term clinical follow-up of the case. The patient's parents were informed that this case would be submitted for publication.
CASE REPORT
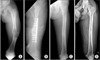
A 12-year-old boy presented with painful swelling on his left thigh after being kicked by his friend. Plain radiography revealed a concentric cystic lesion with cortical thinning and ballooning in the mid-portion of the femoral shaft accompanied by a pathologic fracture (Fig. 1A). The cystic lesion was extensile without a periosteal reaction. The patient underwent curettage of the cystic bone lesion and autogenous bone grafting, followed by open reduction and internal fixation for the pathologic fracture (Fig. 1B). Intraoperative biopsy revealed a unicameral bone cyst (Fig. 2) and, therefore, it was decided to continue close observation of this case without any further intervention. Two years after surgery, plate removal was performed based on radiographic evidence of complete healing of the cystic bone lesion (Fig. 1C). Although 1.5 cm femoral shortening was initially noted after surgery, the leg length discrepancy appeared to have increased with age. Therefore, the patient was scheduled for annual follow-up until skeletal maturity. At the age of 19 years, no recurrence of the cyst was seen on plain radiographs of the femur (Fig. 1D), and the final leg length discrepancy was 3.5 cm (Fig. 3). The patient complained of abnormal gait and posture resulting from the 3.5 cm discrepancy, for which lengthening of the shortened femur was planned in the near future.
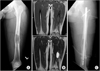
At the age of 20 years, 8 years after the initial surgery, the patient complained of pain in the left thigh. A review of his plain radiographs revealed an impending pathologic fracture caused by a recurrent simple bone cyst in the left femur (Fig. 4A). Magnetic resonance imaging (MRI) scan demonstrated a 6.6 cm × 3 cm × 3 cm-sized, well-defined cystic lesion in the left distal femur (Fig. 4B). Comparison of the radiographs and MRI findings revealed the presence of a linear pathologic fracture accompanied by a periosteal reaction. For treatment of the fracture, curettage and autogenous bone grafting combined with internal fixation using an intramedullary nail (Fig. 4C) were performed. One year after the second surgery, the lesion was stabilized despite cortical thinning and ballooning of the femur (Fig. 5A). Therefore, lengthening of the left femur was carried out with an application of the Ilizarov apparatus over the intramedullary nail to treat the cystic lesion and limb length discrepancy simultaneously (Fig. 5B). Corticotomy was conducted at the level of the proximal femur in order to avoid stress on the cystic lesion. The femur was lengthened by 3.4 cm, and the external fixation index was 11.7 day/cm. Subsequent follow-up was conducted on a regular basis. For 20 months after the lengthening with the Ilizarov apparatus, no evidence of recurrence was observed (Fig. 5C). Intramedullary nail removal was done 30 months after the Ilizarov procedure (Fig. 6A). At 1 year after the hardware removal, there was no radiographic evidence of recurrence of the bone cyst and limb length discrepancy (Fig. 6B).
DISCUSSION
There are few reports on unicameral bone cysts with diaphyseal origin. Based on the reported incidence, a cystic lesion in the diaphysis of the femur in older children as in our patient is more likely to be monostotic fibrous dysplasia rather than a unicameral bone cyst.5) In general, diaphyseal unicameral bone cysts originate near the growth plate and migrate from the metaphysis to the diaphysis during skeletal growth.3) However, the lesion in our patient recurred at the same location as the previous lesion after reaching skeletal maturity, suggesting that the lesion originated from the diaphysis rather than the metaphysis.
Bowen and Morrissy6) reported that development of a unicameral bone cyst is affected by extrinsic factors such as the periosteum rather than the osseous structure itself in a case report of a patient who had recurrence of a unicameral bone cyst in the proximal fibula following a total en bloc subperiosteal resection. In our case, the lesion recurred after complete healing with an intra-lesional osseous procedure, curettage, and bone graft. Therefore, it seems that extraosseous structures may contribute to the development of simple bone cysts. In our case, there was no evidence of recurrence for 8 years after curettage and bone graft, but cystic invasion suddenly developed within 1 year. Our finding suggests that the occurrence of cystic lesions can be triggered by acute induction factors acting on an underlying anatomic variation rather than a chronic course of gradual progression from a small lesion.
The treatment method for unicameral bone cysts depends on their location and the patient's age. Due to their variable biologic behavior, there is presently no agreement on the standard treatment of unicameral bone cysts. A wide spectrum of methods are available from minimally invasive techniques such as aspiration and steroid injection to more aggressive open techniques. In our case, we performed curettage and autogenous bone grafting combined with internal fixation because both the initial and recurrent lesions presented with pathologic fractures. The method of internal fixation is also different according to the presence of the growth plate.
Tsuchiya et al.7) stated that external fixation is an effective technique for correcting deformities and limb length discrepancies produced by benign bone tumors. Jesus-Garcia et al.8) described an Ilizarov apparatus technique performed on 10 patients with Ollier disease. In the study, the treatment results were excellent and the external fixation technique led to conversion of the abnormal cartilage into histologically mature bone. In our patient, gradual lengthening was performed using the Ilizarov apparatus in order to correct the limb length discrepancy and to promote healing of the cystic lesion. Enhancement of the healing process was observed after Ilizarov lengthening in the patient. This finding suggests that the increased blood supply after distraction osteogenesis may affect cystic lesions.
Limb shortening resulting from unicameral bone cysts has been reported in many previous studies. The pathogenesis of limb shortening as a complication of this lesion is not clear, and several theories have been suggested. The major etiologic theories are associated with epiphyseal plate invasion by forming cysts, pathologic fractures, and iatrogenic damage after treatment.9) Although our patient did not show epiphyseal plate involvement, limb shortening progressed with age. Glowacki et al.10) reported two cases of limb shortening in patients with diaphyseal unicameral bone cysts; however, they did not propose a possible cause of the diaphyseal involvement. The association between limb shortening and diaphyseal unicameral bone cysts needs to be investigated in further research.




 XML Download
XML Download