

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Meniscal allograft transplantation has been performed to prevent development of arthritic degeneration in meniscus deficient knees. Despite the favorable short-term clinical outcomes, long-term results have been less satisfactory.1) Verdonk et al.2) reported that follow-up magnetic resonance imaging (MRI) demonstrated partial extrusion of the meniscal allograft in the majority of patients at a minimum follow-up of 10 years. Extrusion of the meniscus is a well-known risk factor for development of osteoarthritis.3,4) Therefore, during every surgical step of the meniscal allograft transplantation, our best efforts have to be focused on prevention of extrusion of the meniscal allograft. Recently published articles emphasized the importance of anatomical placement of the lateral meniscal allograft to decrease postoperative extrusion.56) Here, we present a patient who underwent a lateral meniscal transplantation using a wire that was formed to the contour of the allograft for correct graft placement.
CASE REPORT
A 15-year-old girl presented with sudden pain and sense of giving way of the right knee for 1 week. She underwent total meniscectomy for the lateral meniscus at another hospital 8 years ago. Physical examination showed mild effusion, no joint line tenderness, and negative McMurray test. Her knee was stable and showed a full range of motion. Radiographs and MRI showed a displaced, large osteochondritis dissecans in the lateral femoral condyle. Autogenous osteochondral grafting using multiple plugs was performed immediately, and lateral meniscal transplantation was undertaken 5 years after the osteochondral grafting.
For meniscal transplantation, the patient was positioned supine on the operating table and the right knee was placed in the figure-of-4 position. The size of the meniscal allograft was measured using the radiographic method proposed by Pollard et al.7) After thawing the lateral meniscal allograft, redundant soft tissues of the allograft were excised carefully and a 9-mm bony bridge connecting the anterior and posterior horns of the lateral meniscal allograft was prepared. A 1-mm wire was bent along the medial border of the bony bridge and the periphery of the lateral meniscal allograft (Fig. 1). The prepared wire was introduced through the lateral mini-arthrotomy while the patellar tendon was retracted medially. The straight part of the wire was placed along the lateral tibial spine (Fig. 2A). However, some portion of the round part of the wire was extruded from the anterolateral margin of the lateral tibial plateau. The straight part of the wire was moved more medially and rotated internally. The round part of the wire was placed accurately along the anterolateral margin of the lateral tibial plateau (Fig. 2B). The direction of the straight portion of the wire was marked with electrocautery. After removal of the wire, a bony trough was made along the marked line using a U-shaped chisel. The rest of the transplantation procedure of the lateral meniscal allograft was done in the usual manner.
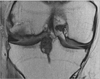
At 1 year after surgery, she had no pain or effusion or pain during McMurray test on the right knee. Her Lysholm score was 86 and Tegner activity scale was 4. Follow-up MRI showed low-signal intensity of the midbody of the allograft that was positioned adequately without extrusion (Fig. 3).
DISCUSSION
The anterior horn of the lateral meniscus always blends with the anterolateral bundle of the anterior cruciate ligament.8) The posterior horn inserts more centrally than the posterior aspect of the lateral tibial spine. The anterior aspect of the lateral tibial spine can be visualized with a mini-arthrotomy. However, the posterior aspect of the lateral tibial spine can be barely seen, because it is mostly obscured by the anterior cruciate ligament.9) Anatomic complexity of the insertions of the horns of the lateral meniscus can lead to a relatively lateralized transplantation of the meniscal allograft. It is also impossible to know the exact rotation of the allograft during transplantation even under the fluoroscopic control. A recent study demonstrated that an externally rotated keyhole of the graft is a factor responsible for midbody extrusion.6) The technique descried in this report using a wire that is shaped to conform to the contour of the lateral meniscal allograft will help surgeons to place the graft more accurately and anatomically. For this technique, however, the use of a thin wire should be avoided to prevention distortion during insertion via a mini-arthrotomy.


 XML Download
XML Download